Update on previous post: Hubby replied to Dave’s email. He’s awesome, is (once again) Captain of Team D Beats C, and I hope he writes about his experiences as a caregiver and spouse of someone living with cancer someday. I also called AACR and spoke to Josh, a very nice and caring human being who agreed that the response I first received was not appropriate or kind. He asked that I forward my correspondence to him so that he could look into it.
He also expressed heartfelt wishes for me as I deal with another round of breast cancer.
Later, I received a call from Sheraine, Customer Service Team Lead from Compusystems. She offered an apology and heartfelt wishes for a speedy recovery. She assured me that there are scripted responses that are available and appropriate for cases of illness and they would make sure those responses are used in the future.
A little kindness goes a long way. I’m pleased with the outcome.
I didn’t plan on writing two blog posts in one day, but here we are. Because of my second diagnosis with breast cancer, I have to adjust my life and schedule to accommodate surgery, reconstruction, and other treatments. I had planned to attend the annual American Association for Cancer Research Annual Meeting in April so I could present my research on molecular regulation of breast cancer bone metastasis, network with colleagues, patients, survivors, and policy makers, and learn about the latest advances in the field.
Cancer has robbed me of that opportunity.
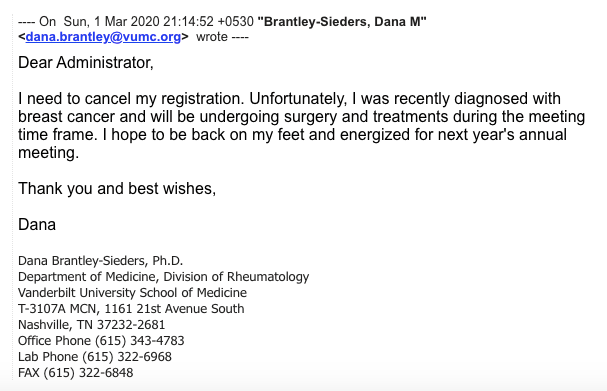
Since I’d already registered, I contacted AACR to let them know what was going on and to cancel my registration. Here’s what I wrote:
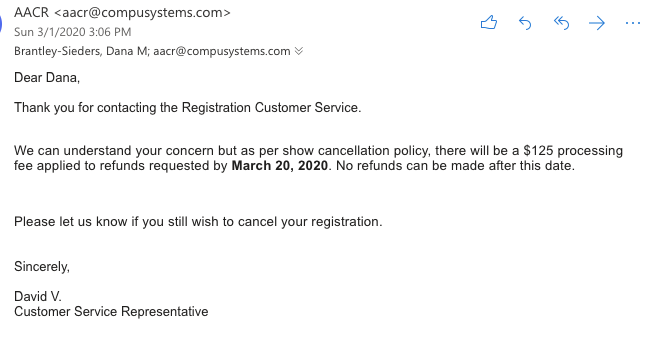
Short, sweet, to the point. I didn’t expect a reply until next week, but, to my surprise (and based on the tone of the reply, horror), I received a reply within a few hours:
So, after writing the American Association for CANCER Research to let them know that I cannot attend the meeting because I have CANCER, that’s the stone cold, insensitive, shitty reply I received. I could’ve let it slide, but, as I note in my response, I’m soooooooo done with bullshit at this point.
Here’s my reply (copied and pasted since it’s too long for a screenshot):
Dear David,
Wow. Just wow.
Two years ago, I would have just let this slide, been “nice” and “quiet” without causing trouble, like all women are taught to do. But two years ago, I was diagnosed with breast cancer. And, as of last week, my breast cancer is back. As such, I have neither the time nor the energy for bovine fecal material. That the current bovine fecal material is coming from the American Association for Cancer Research, an organization I’ve supported since my days as a graduate student (member 1998-present), just after a second diagnosis with breast cancer, makes it all the more horrible.
As I noted in my request, I have cancer. I will likely be undergoing surgery for the third time during the annual conference, which means cancer has cheated me of the opportunity to present my own research findings on breast cancer metastasis to my peers. Cancer will also steal time from my research, my family, my friends, and my life. So, in response to, “Please let us know if you still wish to cancel your registration,” um, yeah. Did you think I’d suddenly change my mind, or that my cancer would suddenly be all better so I can totally go to the meeting – my bad? What kind of stupid, insensitive question is that? Seriously, I have people who despise me who wouldn’t be that stone cold. Do you need proof of my diagnosis? I have CDs full of scans from my six biopsies and two lumpectomies. Do I need a doctor’s note? You can check out my blog where I’ve been documenting my story in an effort to let patients going through the same struggles that (a) they’re not alone, (b) knowledge is power so here are accessible data you can use to make informed healthcare decisions, and (c) to be a liaison between research and patients/survivors so the public understands how important our work is and so they’ll engage to help us better meet their needs. www.talkingtatas.com.
You’d best believe I’ll be blogging about the AACR responding to the news that I have cancer and cannot attend the annual meeting with it’ll cost you $125. No “I’m so sorry for what you’re going through.” No, “What can the AACR do to support you during this difficult time.” Just, “We can understand your concern.”
You can understand my concern, you say. With all due respect, no, unless you’ve had cancer, you absolutely, positively cannot understand even a fraction of my concerns. Unless you’ve been hit by the sledgehammer of shock upon hearing those three horrible words, you have cancer, unless you’ve had to tell your spouse, your children, and your mother that you’ve been diagnosed with a deadly disease, unless you’ve endured the pain of surgery and recovery, the burns and fatigue induced by radiation, the indignity of estrogen suppression therapies that forever change you and your relationship to your body, unless you’ve endured sleepless nights wondering if you’ll live for another 5 years, 10 years, 15 years, and if/when cancer might come back and kill you, you have NO IDEA about my concerns. That’s completely insensitive, condescending, and wrong on so many levels.
But please, by all means, take the $125. You certainly need it more than I do. I don’t need to think about insurance deductibles, medication, bills to support myself and my family.
And one last thing – you don’t get to call me “Dana” in a response like the one you offered. It’s Dr. Brantley-Sieders to you.
A little consideration, human decency, and kindness can go a long way. Coldness, disregard, and insensitivity can, too. Badly done, AACR. Badly done.
I’ve come to terms with the fact that I’m not done with breast cancer yet. But I don’t have to like it, and I don’t have to pretend that I’m entirely okay. I need help. Still in therapy, meeting with my care team on Thursday to come up with a game plan to get rid of this stupid little 6 mm bastard of a tumor, and then meeting with the plastic surgeon the following Monday to discuss Tits 3.0.
It’s a lot. What’s keeping me sane right now, aside from my family, Netflix Comedy Specials, and cat videos on Facebook, is my work. Y’all, I get to kill breast cancer cells ALL THE TIME in the lab. It’s so cathartic and gratifying. I wish with all my heart it was as easy to kill cancer cells in patients as it is in little plastic dishes. It’s not, but what we discover in little plastic dishes could eventually lead to the next cancer therapy.
The message is clear – DIE BITCH ASS CANCER CELLS!
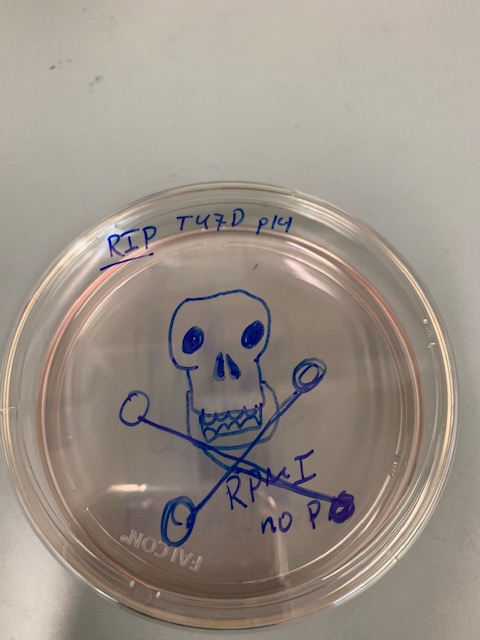
My amazing student, who’s working with cancer cells that are similar to mine (hormone receptor positive), saved a plate for me. Not only did she save a plate, she decorated it with an adorkable “destroy me” tag that made me giggle snort.
I adore her.
Naturally, we decided to video me killing cancer cells.
Videography credit Kalin Wilson
As noted in the video, please for the love of your health, do NOT drink hydrogen peroxide to kill you tumor. It’s #toxic and not in a way that will target your cancer. But, as you can (hopefully) see, it stresses out the cells in the dish, overwhelming their defenses against oxidative stress to the point of death.
But, having the power to kill tumor cells that are similar to those growing in my body helped me on a psychological level. And if any patients or survivors want me to kill cancer cells like yours in the lab, I’m down! Hit me up. I can use chemo drugs, approved and experimental cancer drugs, peroxide, detergents, soda (it totally works), you name it. Let’s get creative!
I learned so many new things today at Patient Advocacy Orientation! My best days are when I’m learning new things. It’s one of the things I love best about being a scientist, and it’s a great foundation upon which to build for my new work as a Patient Advocate.
What exactly are advocates and what do they do? In terms of Research Advocacy Programs, advocates are disease survivors (cancer survivors in my case), caregivers, and members of the community who provide the patient perspective to researchers to help shape the nature and direction of cancer research and patient care. Their role is critical, as they serve as a voice for patients, helping investigators tailor their research with patients concerns in mind – not just in terms of outcomes and sound science, but also in terms patient comfort, respect for patient rights and dignity, and beneficence. This means making sure the goals of research are focused on and aligned with serving patient needs and improving outcomes and quality of life.
This seems pretty intuitive, and I believe most investigators are truly committed and passionate about doing research that will make a difference, be it developing new treatments, better diagnostic tools, reducing side effects of existing treatments, and improving survival and quality of life for patients. I certainly was and am. But most investigators don’t experience what patients do – except in cases like mine where researchers become patients and survivors. My experience certainly changed my perspective, which is why I want to share what I’ve learned with both the research and survivor communities.
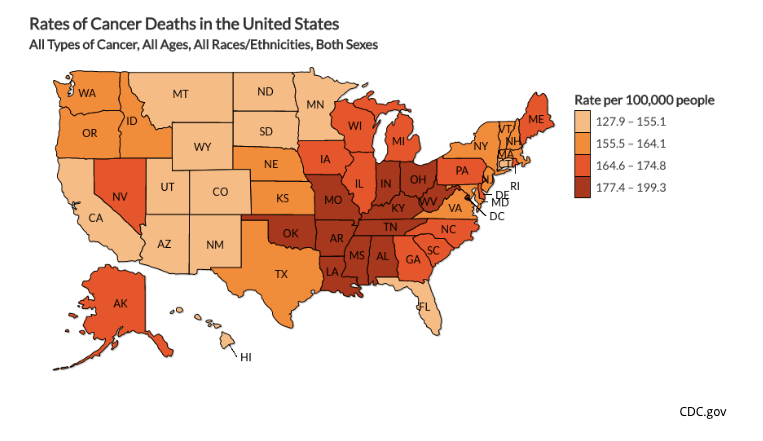
That mission became more urgent for me today in the face of some jarring statistics. Tennessee and the surrounding regions have some of the highest cancer death rates in the United States.
Comparing the map above to the map below that shows new cancer cases diagnosed by state, incidence, the frequency with which cancer occurs, doesn’t fully explain higher death rates.
My heart sank when I saw these data, and really drove home my privilege. I am well-educated, have a high socioeconomic status, have access to insurance coverage and some of the best health care available in the United States, and I have inside information based on my work as a breast cancer researcher.
I’m lucky. Far too many of my fellow Tennesseans and Southerners are not. My Institution and Affiliated Cancer Center serve this region. I want to be a part of better serving patients in this region, which will be a HUGE focus of my advocacy work.
What will this work involve? One of the ways I think I can be of use is by helping recruit patients for clinical trials. According to what I learned today, many promising new drugs do not make it through Phase III clinical trial testing* due to failure to accrue enough patients to sufficiently test their effectiveness. That’s such a shame and missed opportunity. Of course, there are many barriers for patient participation in clinical trials – fear/lack of understanding; lack of access due to barriers to travel/transportation, unmet childcare needs, inability to take time off work, etc.; disparities that make minority populations reluctant to participate**. While I am not in a position to combat access to trials, I am in a position to serve as a liaison between patients and clinical researchers accruing patients for trials. I can help educate potential trial participants in the process, assure them of their rights (including the ability to stop participating at any time), alleviate fears through helping patients understand the benefits and how they might be helping a great number of future cancer patients. I am also working with African American advocates and other advocates of color to understand and be sensitive to those communities, their histories, and their needs.
Those needs are great, particularly in terms of breast cancer outcomes. African American women diagnosed with breast cancer have lower overall survival rates compared to white women. Finding out why is crucial for closing the gap. Increasing African American participation in clinical trials is a key part of that process.
*I’ll cover clinical trials in more detail in a future post. Click here to learn more now. Phase III trials test drugs that have already been proven safe and promising in terms of effectiveness.
**African Americans remember the horrific abuses perpetrated by scientific investigators, including those in charge of Tuskegee Study of Syphilis – which resulted in hundreds of African Americans being denied treatment in order to study the long term effects of untreated syphilis
Essential oils. They’re EVERYWHERE! Articles and posts touting their alleged benefits are all over social media, some news media, and the Internet. A Google search I performed today yielded 1.7 billion results. 1.7 BILLION! Yup, there’s a LOT of buzz about the wonders and medicinal benefits of essential oils.
And almost all of it 100% certified Grade A Bullshit.
This post is dedicated to debunking one of my least favorite bullshit woo woo scams (second only to homeopathy). And I will do so with the power of science and snark, because that’s just who I am as a person.
So what are essential oils? They are oils purified from plants and carry the aroma of the source from which they are extracted. Their name comes from the fact that they are thought to contain the essence of their source, and they smell pretty good thanks to terpenoids, aromatic organic compounds produced by plants that often function as chemical protection against herbivores, insects, and microbes. They also serve as attractants for pollinators, seed dispersers, and in mediating plant–plant and plant–microbe communication. Humans enjoy them because they smell and in some cases taste really good. Sadly, allergies prevent me from enjoying the florals, but I enjoy herbals and fruit oils in a wide array of products – cosmetics, soaps, perfumes, lotions, bath products, and many food items. They’re just nice.
Fresh herbs and oils, wooden table background – we smell good and taste nice!
But do they have any medicinal value? What about medicinal value when it comes to cancer? Part of the issue with answering this question involves the (lack of) regulation when it comes to production and testing. The concentration of active chemicals in extracts can vary widely from plant to plant, which parts are processed (different concentrations in leaves, flowers, stems, and roots), which season the plants are harvested, which strains are sourced, etc. Without consistent batches subjected to quality control to assure consistent concentrations of active chemical components (like terpenoids), and without rigorous, scientific studies, we can only rely on anecdotal evidence and (often misleading) claims from suppliers. Some efforts are being made by the WHO for quality and safety evaluation of herbal products, including chemical fingerprint analysis*. Much like vitamins and supplements, which are not subject to the same rigorous FDA standards for safety and efficacy (how well it works) as drugs, essential oils fall under the category of “safe for their intended use,” which does not involve use as medical treatments. They’re considered safe until proven otherwise, a MUCH lower standard than FDA approved drugs.
More importantly, they are (by fairly low standards) rated for safety, but not for EFFICACY. That would require clinical trials and rigorous testing.
Should we be researching them? Sure! Some pre-clinical studies involving cultured cells (cells grow in a petri dish under laboratory conditions) and animal (primarily mouse) models have been published. A systematic review of the literature from 2014 to 2019 identified 79 studies that fit inclusion criteria – including studies investigating essential oils with anti-microbial and immunomodulatory (affects the host immune response) properties, nutrition studies, studies with controls and proper statistical analyses. Of those studies, many documented the anti-microbial (bacteria fighting) and anti-fungal (fungus fighting) properties, antioxidant properties that may help slow food spoilage, and anti-inflammatory properties in laboratory and agriculture models. And, in some preclinical studies, high doses of essential oils can kill cancer cells in culture in a laboratory setting. Does that mean they’ll do the same thing in humans? Not necessarily. See my post on turmeric.
Just for perspective, it’s pretty easy to kill cancer cells in culture in a laboratory setting. I once killed a dish by accidentally leaving the cells in phosphate buffered saline instead of growth media. Yes, salt water can kill cancer cells in culture. So can many drugs, but the majority of compounds with anti-cancer activity in cultured cancer cells and mouse models are not effective in human clinical trials. So, the jury is out on whether or not the active ingredients essential oils can help treat cancer. And inhaling the pleasing aromas produced by essential oils may effect mood, but it doesn’t do anything to thwart cancer growth, survival, or invasion.
These observations definitely warrant more laboratory investigation, but as of this post, there is no evidence that essential oils fights cancer when inhaled or ingested or delivered in any other way into the human body. Advertisements by scammers like the ones listed below are lies:
These are some of the top hits under a Google search for “treating cancer with essential oils.” As is my standard policy, I will not share links for woo woo. The misinformation and outright lies are not only infuriating, they can prove deadly for patients who skip standard therapies in favor of alternative “therapies.” The stats are heartbreaking. In a Yale School of Medicine study (link to original publication here*), “patients who used alternative medicine in place of standard evidence-based medicine had a death rate 2.5 times higher than patients who received standard evidenced-based therapies.”
Women with non-metastatic breast cancer who opted for alternative “medicine” were ~ 6 times more likely to die within 5 1/2 years compared to women who received standard of care therapy. This is a small study – 281 patients – and captures data from patients who disclosed their decision to follow alternatives versus standard of care. It doesn’t include patients who do not disclose or discuss this with their health care providers, so the numbers could actually be higher.
For more information on aromatherapy – separating fact from fiction – click here. Check out this article, too. Bottom line: much like cannabis, essential oils may offer relief from the side effects of standard of care treatments, but they cannot cure cancer nor should they be used as a substitute for standard of care. Complimentary alternative medicine is fine, as it compliments proven therapies, but not on their own.
*Access to this article is limited by a paywall. If you want to read it for yourself, hit me up and I’ll send the PDF.
One of my favorite outreach activities is volunteering at public schools. Over the years, I’ve had the opportunity to speak to and work with elementary, middle, and high school students – doing everything from dry ice demonstrations, mini anatomy labs with fixed mouse organs, microscopy labs with tissue sections, and career talks. Most recently, I visited a local MNPS high school to talk about cancer biology (click here to see the slide show and an explanation).
It was AWESOME!
First of all, I was super impressed by how much these young people already knew! They’re studying cell biology and cell division right now, which worked well for my talk about how errors in DNA replication, mutations, and failed repair after damage leading to amplifications and deletions contribute to cancer. We used cell cycle regulation as an example, talking about oncogenes (drive cancer growth) and tumor suppressors (normal braking system for growth – lost in many cancers) that encode cell cycle regulators. They already knew much of the background, including how the cell cycle is controlled, the steps involved, and some of the proteins that regulate it. They also knew a lot about carcinogens (e.g. cigarette smoke, ultraviolet radiation from the sun, certain chemicals), treatments (chemotherapy and radiation), and certain types of cancer including breast, lung, and colon cancer.
Secondly, they were engaged and asked a LOT of questions. It made the presentation much more fun and interactive, and it gave me quite a bit to think about. There were, of course, questions I could not answer off the top of my head. But I promised the students I would look up answers to their questions and send the answers to their teacher. These are some of those questions:
1. What is the rarest form of cancer?
The latest statistics I could find from the American Cancer Society are from 2017. According to the data they gathered, the rarest cancers diagnosed in the adults (20+ years old) in the United States include cancers of the trachea, Kaposi sarcoma (this one is interesting because it led to the discovery of HIV – when more of these cancers cropped up in young gay men in the 1980s, it led investigators to start studying this population to identify the cause), lip, nose cavity and middle ear.
2. Can cancer in a transplanted organ spread to a new host?
This has actually happened! In 2018, it was reported that a 53 year old woman who died from a stroke and had no known medical conditions at the time of her death (including screens for cancer) had her organs transplanted into at least 5 recipients. The patient who received the heart died shortly after transplant from unrelated causes, but a year and a half later, the patient who received lungs from the donor became ill and was found to have breast cancer cells in her body with DNA that matched the original donor. She died shortly after. The patient who received the donor’s liver developed breast cancer in the transplanted organ in 2011, was treated, but died of a recurrence in 2014. The patient who received the donor’s left kidney developed and died from breast cancer in 2013 (six years after transplant), and the patient who received the donor’s right kidney was diagnosed with breast cancer in his kidney cells in 2011 – they were able to remove the tumor from the kidney, and after treatment the patient lived 10 years cancer free (at the time of reporting).
This phenomenon is very rare, however, and most of the time cancer in a potential donor can be detected by screening before organ harvest.
Apparently, clams do get cancer. Even worse, for at least one type of cancer, the cancer cells from one clam can travel to another clam through water and grow in the new host. Yikes!
Cancers have been documented in reptiles, but they are much more under-studied than mammals and other animals. More research may be done to better study the link between cancer and metabolism, since metabolism is lower/slower in ectotherms (cold blooded creatures) than endotherms (warm blooded creatures).
Interestingly, elephants and naked mole rats rarely, if ever, get cancer, and ongoing studies into their physiology and genetics could help us figure out why and how we can use the knowledge to prevent cancer in humans.
4. Can babies be born with cancer?
It is rare, but it can happen. There have been reports of babies born with neuroblastoma, leukemia, and teratomas.
5. When did people start getting cancer?
(I actually knew part of the answer to this one, but it was fun to dig a little deeper)
The world’s oldest recorded case of cancer came from ancient Egypt in 1500 B.C., and it was recorded that there was no treatment for the cancer, only palliative treatment (relief of pain and suffering). Cancer has been with us much longer, though, given that bone cancer (osteosarcoma) has been detected in fossils from early hominids dated to 1.7 million years ago. Similar tumors have been found in fossils from dinosaurs and even from ancient turtles that lived 240 million years ago!
Got any questions for me? Send them! I’ll do my best to find the answers and more information. Knowledge is power! Hit me with your burning questions – the weirder the better!
If I had a quarter for every time someone told me they read that some discovery was the cure for cancer over the past twenty years, I could afford to take that trip to Tahiti I’ve been dreaming about. Science and the news media have an interesting relationship. On one hand, it’s always great to get coverage for advances in science. It keeps the public informed and engaged, which in turn means more interest and research dollars for laboratory and clinical investigation.
On the other hand, the news media gets a lot wrong, and that’s actually bad for keeping the public informed and for public perception and expectations, especially when it comes to complex diseases like cancer.
Take, for example, recent press coverage of a discovery related to tumor immunology – the study of how we can harness a patient’s own immune system to fight their cancer. It’s a hot topic. In fact, two leaders in the field, James Allison and Tasuku Honjo, were awarded the Nobel Prize for Physiology and Medicine in 2018 for their discovery of a new cancertherapy by inhibition of negative immune regulation, which led to the development of several drugs currently available to treat certain types of cancer. More recently, a paper published in Nature Immunology captured the attention of news outlets, leading to headlines like:
The first outlet, Science Alert, gets it right. The discovery is indeed remarkable, and the note about the ability to kill several cancer types in the laboratory is an accurate representation of what the study showed (my only issue with the headline is the clunky construction – discovery doesn’t kill anything – but that’s just me being nitpicky). The study tested activity of T-cells, part of the immune system that kills cells that have been infected by pathogens (bacteria and viruses) that can also be engineered to target cancer cells in cell culture (cells grown on a plastic dish in the laboratory) and in mouse models (mice engineered to make tumors or transplanted with tumors). This is an essential first step for the development of new therapies, but it is a far cry from being ready to use in patients, as the BBC News and Newsweek headlines might lead people to believe.
But can switching to these new T-cells save me 15% or more on car insurance?
I get why this happens. In the age of 24 hour news cycles, multiple media outlets (online, television, radio, and print), sensational headlines sell. The idea that a new discovery could treat all cancer (a far-fetched notion given that cancer is a collection of diseases that are unique and adaptable) sounds exciting. It captures public interest, especially in patient and survivor communities. But those headlines are misleading, and that’s a problem. While most of the public will forget the specifics, some will look at the next headline related to cancer and think, “Wait, didn’t they find something that’s going to cure cancer soon? What happened to that?” The false promises made by these headlines can give the public the idea that most of what cancer researchers are doing is a waste since the sensationalized discoveries didn’t live up to the hype.
So, let’s look beyond the headlines and delve into the study. What did the investigators do (experimental methods and models), what were the results (data), and what do the results tells us (interpretation)?
To begin, we need a basic understanding of how T-cells (one of many cell types in the immune system) function in fighting disease. They are part of the adaptive immune response – meaning they are selected to attack specific pathogens based on unique proteins and, as noted in the paper, metabolic by-products, produced by target cells.
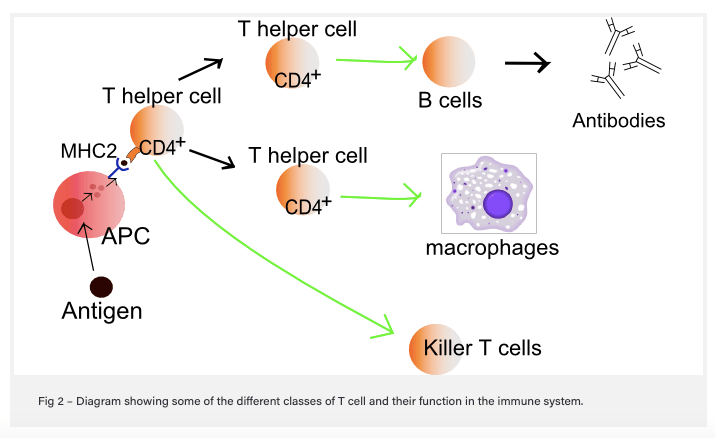
Here’s how it works: when a cell becomes infected with a bacteria or virus, the infected cell takes some of the foreign proteins (antigens) from the bacteria or virus and displays it on the cell surface in combination with proteins (major histocompatibility complex [MHC] – also known as the human leukocyte antigen [HLA] system in humans] that communicate with immune cells. Surveillance cells like macrophages, which can “eat” infected cells, also do this, and these cells are known as professional antigen-presenting cells (APC). Helper T-cells in the vicinity that recognize the antigen communicate with B-cells, which make antibodies to attack cells that are infected and display the same antigen, and with Killer T-cells (cytotoxic), which bind to and destroy infected cells that express the same antigen. In order to bind to the antigen/MHC complex, T-cells like the killers use cell surface protein receptors (T-cell receptors [TCR]). This is how conventional T-cells function.
Now, on to breaking down the actual published study!
The new study focused on unconventional T-cells that do not recognize protein antigens bound to MHC on antigen-presenting cells. These specialized T-cells normally sense bacterial metabolic by-products bound to the evolutionarily conserved, monomorphic MHC class 1-related protein MR1 – a fancy way of saying that the MR1 cell surface receptor is similar across species (evolutionarily conserved) and come in one form (monomorphic). This types of T-cell was identified from an experimental screen used to identify tumor-educated (e.g. grown in response to tumor cells) T-cells that recognize and kill cancer cells in a petri dish in a non-MHC (MHC mismatched) manner. This is important, since MHC/HLA are some of the most variable proteins within and between people and therefore not easy to develop and exploit as a universal anti-cancer treatment. The T-cell clone identified, called MC.7.G5, was able to kill cells from different types of cancer (lung, melanoma, leukemia, colon, breast, prostate, bone and ovarian) with different MHC/HLA types in petri dishes without harming normal, healthy cells.
Using other molecular biology techniques, the investigators determined that the T-cells that can recognize and destroy cancer cells in a non-MHC-dependent manner. Rather, the cancer-killing T-cells had receptors (TCR) that bound to MR1 plus a cancer-specific cargo (antigen – possibly a non-protein antigen) that has not yet been identified.
To see if these T-cells kill cancer in a whole animal model system, the investigators transplanted human leukemia cells into mice that lacked a functional immune system along with MC.7.G5 T-cells. The mice that received the MC.7.G5 T-cells showed evidence of reduced leukemia cells relative to controls, and when they tested leukemia cells that did not express MR1, the anti-leukemia activity went away – this is an important control, because it shows that MR1 is, in fact, necessary for MC.7.G5 T-cell activity. Finally, the investigators purified T-cells from actual patients with stage IV (metastatic) melanoma, engineered the purified T-cells to express the same T-cell receptor as MC.7.G5 cells, and tested the ability of these engineered T-cells to kill melanoma cells in a petri dish. The cells engineered to express the MC.7.G5 TCR killed melanoma cells from patients with similar or dissimilar HLA, but not melanoma cells that didn’t express MR1.
So what does all of this mean?? The significance is that T-cell subtypes that may be present in most humans and similar in most humans can recognize and destroy a variety of different cancer cells in laboratory models. It is exciting because, if validated in more laboratory research models (and if these types of T-cells are observed in actual cancer patients, including those with better outcomes), it could give scientists and physicians a new therapeutic tool to use in the clinic.
BUT
Before that can happen, a LOT more work has to be done, including:
Figuring out what cancer-specific antigen MR1 binds to – this is super important, since the presence of whatever that antigen might be would have to be detected in actual cancer patients before trying out these new T-cells in clinical trials.
Long-term studies to see if the health of the animal is affected by exposure to T-cell therapy. One of the challenges with anti-tumor immune therapy is the risk that patients might develop an auto-immune disease (e.g. immune cells will recognize the patient’s own healthy cells and attack, like what happens in Type I diabetes and Rheumatoid Arthritis). Remember, cancer cells are normal cells gone rogue, and they may be similar enough to normal cells within the body to trigger an unwanted immune response.
Getting the T-cells to go to the tumor, infiltrate it, and kill enough tumor cells is also a challenge. It’s a challenge with all immune therapies. Tumors that normally have a lot of T-cells hanging around (“hot” tumors) generally respond better to existing immune activating drugs, but many tumors don’t have a lot of T-cells that infiltrate (“cold” tumors”). These new T-cells can only be effective if they can get to the tumor, and tumors often adapt to evade or repel immune cells.
Finally, just because something works in laboratory models, like cells in petri dishes or even laboratory mice, doesn’t mean it will work in humans. We’ve been successfully killing cancer in petri dishes and mice for decades, and the clinical trials graveyard is full of therapies that showed great promise in the laboratory only to fail in clinical trials – some of those cases may be due to trial design, especially in early trials where patients weren’t always screened for the target. But other cases are probably due to our inability to replicate human disease fully in models that are not as naturally complex. Most mouse models used in the laboratory are inbred (for more on the history behind that, follow this link – yes, I know it’s a Wikipedia link. Wiki isn’t always wrong.). This means we’re using clones in our experiments, and some of those are even more abnormal since they don’t have a functional immune system. The advantage is that we can get more consistent, reproducible results and also that we can get mice without an immune system to grow human tumor cells without rejecting them. The disadvantage is that humans, not being clones, vary widely in their physiologies and responses to therapy. And even when it comes to mouse tumors grown in mice with a working immune system, there are differences in how mouse and human immune systems work – actually, in my experience, laboratory mice are WAY more resilient and resistant to infections than people.
Take home message – look past the headline to the actual data.
It’s a lot of work and requires a fair amount of background knowledge to go to the primary literature and make sense of it, but often enough, the story below the headline can give you enough information to figure out what a study shows, what it doesn’t show, and how close the results are to making it to the clinic.
For example, the BBC News article states that “The findings, published in Nature Immunology, have not been tested in patients, but the researchers say they have “enormous potential”.” I’ll also give the author of this article props for explaining CAR-T cell technology – which is how the cancer-fighting T-cells may be engineered from patient T-cells if the study findings are translated to the clinic. But the headline? Totally misleading.
Same goes for Newsweek, which presents the full headline as: ‘ONE-SIZE-FITS-ALL’ CANCER TREATMENT COULD BE ON THE HORIZON AFTER SCIENTISTS DISCOVER NEW IMMUNE CELL BY ACCIDENT.” Not the accident part – scientists discover stuff by accident all the time, but the idea that this is “on the horizon” gives the impression that it’ll be going to the clinic very soon. Um…not likely. Still, within the article, the author notes, “In mice experiments and in lab dishes, the team showed that a new type of what are known as T-cells could detect a range of cancerous cells, while differentiating them from healthy cells.” That, in a nutshell, is what the investigators actually showed. Headline is still misleading, though.
Bottom line – look BEYOND the sensational headline. It’s purpose is to hook you and get you to click on and read the article (while being bombarded with ads). Dig into the actual article to find out what the new and exciting study shows.
Cancer has been with us since we became human, and probably before, since cancer isn’t common to our species. In a fundamental way, cancer is us. Cancer was once healthy tissue, starting out as a cell in your body fulfilling its function to keep the collective whole, you, functioning. This cell toed the line, divided when it was supposed to, stopped dividing when it was supposed to, differentiated and specialized to perform its function, and if it had remained normal, it might have died when told to do so after that function was fulfilled. Those are three of the hallmarks of cancer: uncontrolled cell division (cells making more cells), failure to respond to the normal programs that put the brakes on cell division, and failure to undergo programmed cell death (die when the time is right).
The process by which a normal cell becomes cancerous is called malignant transformation or carcinogenesis. This video provides an excellent overview of the process.
To understand how cancer forms, we need a basic framework for understanding cellular function and its regulation at the molecular level. Don’t get bogged down in the terms. Cellular function refers to how the cell does its programmed job, how it grows and divides, and how it dies, the same basic life cycle that the human host experiences. Regulation at the molecular level means the plan the cell follows, the blueprint for its growth, function, and death. It starts with DNA, the double helix genetic blueprint in all cells that contains the instructions for the cell’s functions and life plan.
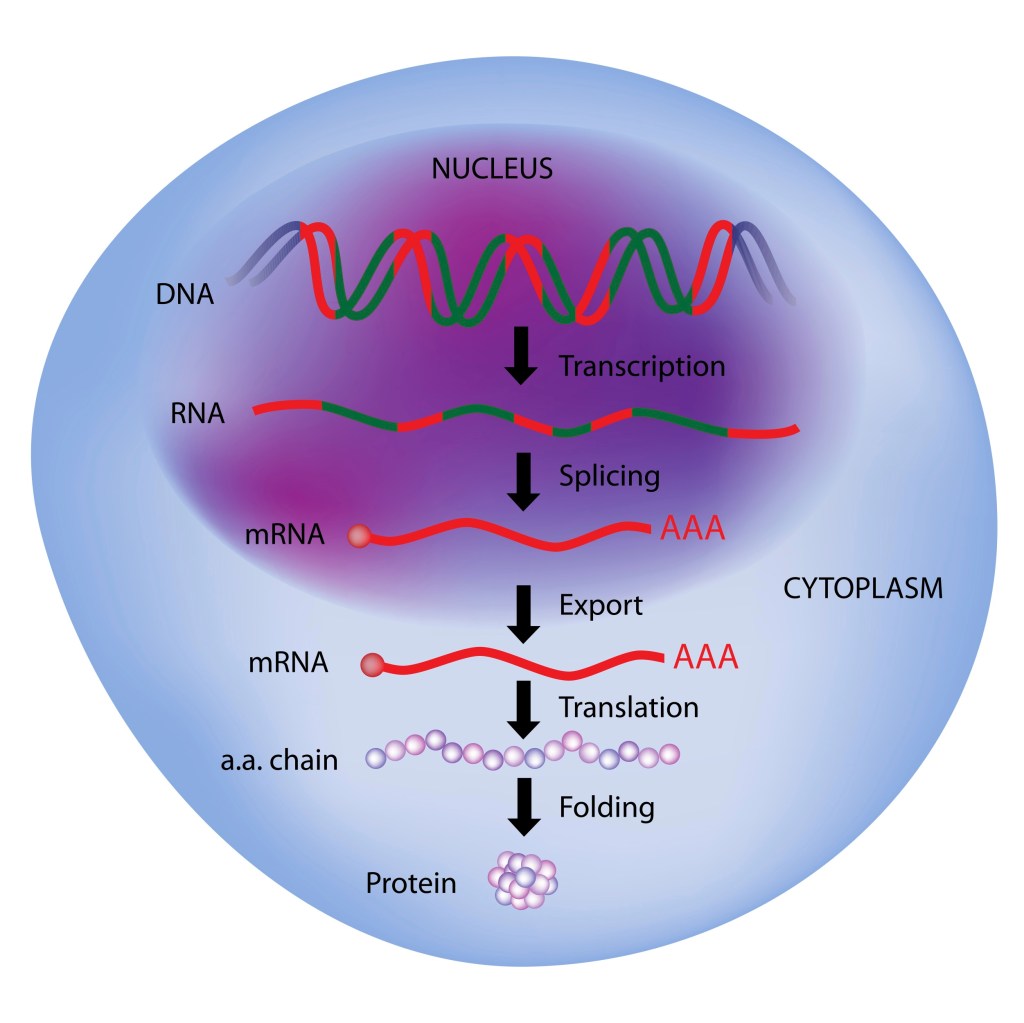
Illustration of the Central Dogma of Molecular Biology – Nuclear DNA is transcribed to an intermediate, called RNA, which is then used as a template for translation into amino acid chains that form proteins. Illustration credit: Shutterstock.
So what does DNA actually do, or perhaps the better question, how does the information encoded in DNA actually instruct the cell what to do? This gets into something call the Central Dogma of Molecular Biology. That’s a fancy title for the way in which the instructions encoded in DNA are used to manufacture proteins, the work horses of cells. Now, when most people think about proteins, they envision a juicy piece of meat or powerful muscles, and the components used to build muscle fibers are proteins. But proteins are much more than that. They are the essential building blocks of cells, which in turn build tissues, organs, and all parts of the body. They can be structural, like the fibers that form the cell’s cytoskeleton and histone proteins that wrap around DNA strands and protect them. They can be functional, forming enzymes that do everything from metabolize nutrients, breaking them down into usable building blocks for building biomass and generating energy for the cell. They also play a critical role in transmitting information within cells and between cells, integrating communication between different parts of the body.
Proteins are made up of chains of amino acids, and the order in which they are put together is determined by the sequence of the portion of DNA that encodes that protein. That sequence is called a gene. But as a matter of practicality, since DNA is housed in a subcellular organelle called the nucleus and therefore inaccessible to the protein production machinery in the cytoplasm, and because the cell needs to protect the integrity of its DNA, proteins are not built using pieces of actual DNA. The portion of the DNA, the gene, that encodes instructions for making a specific protein, is first transcribed into an intermediate molecule, call messenger RNA. Transcriptional machinery within the nucleus unwinds and separates the DNA strands, using one strand to copy the information necessary to build a protein. The messenger RNA molecule is then transported out of the nucleus and used by the protein synthesis machinery to translate the information encoded by the mRNA to protein. That’s the Central Dogma: DNA transcribed to RNA, and RNA translated to protein.
The abnormal growth that is cancer is controlled by abnormal proteins that were once (supposed to be) normal proteins. Most of the proteins that drive cancer are proteins that regulate cellular division and cellular survival, and they fall into two basic categories: oncoproteins and tumor suppressors. Oncoproteins are hyperactive proteins that start out as normal proteins, encoded by normal genes, proto-oncogenes. They become oncogenes due to alterations in DNA: mutations that change the DNA sequence, which in turn changes the amino acid encoded and the function of the protein; DNA repair mistakes that cause multiple copies of genes (amplification) to produce too much of a protein that drives growth and survival; changes in DNA that make the gene more accessible, which in turn causes the cell to make more copies of the encoded protein. DNA damage that causes breaks, which can eliminate genes that normally keep cell growth controlled, can silence tumor suppressors.
Types of DNA damage – if damage is not repaired or is improperly repaired, alterations in DNA (e.g. mutations, deletions, amplifications) that encodes growth and/or survival genes can lead to malignant transformation of a normal cell into a cancer cell.Linkto photo source.
What’s worse is that the longer the cancer grows unchecked, the more mutations and DNA changes it collects. Those alterations and mutations that give the cell an advantage (more growth, better survival, the ability to break away from the tumor mass and spread) make the cancer more aggressive and difficult to treat.
Cancer Formation and Abnormal Growth – Illustration credit: Deposit Photos.
In my next post, I’ll cover the process of malignant transformation of breast cells, which leads to breast cancer.