Use the promo code 22JOYSALE at checkout to get the sale price now through January 6, 2023!
This is a great deal, as you’ll save over $12 on the Hardback and almost $12 on the eBook. Know someone who is going through breast cancer? This would be a helpful gift. Know someone who’s a science loving nerd? They’ll probably like it, too!
It’s day 26 of National Breast Cancer Awareness month! Today, I had the opportunity to appear on the Tampa Reads segment of Fox 13 in Tampa with anchor Linda Hurtado! I was able to share my breast cancer story with a bit about science, about my personal story, and a bit about Talking to My Tatas.
It was a great experience and I hope I convinced some viewers to schedule their mammograms! Shout out to Linda Hurtado, Lisa Emerson, and the rest of Fox 13 News Team!
It’s day 19 of National Breast Cancer Awareness Month! Day 18 was super busy for me with work, doc appointments, and life, so I was unable to post. It happens. But hopefully today’s (late) post will be informative and eye-opening. It certainly was for me.
Sexism, racism, anti-Semitism, homophobia, and all the other prejudices and bigotries that plague humanity exist in science. On the one hand, scientists are rational people who should be objective, but on the other hand, scientists are, well, human. We’re not immune to biases and the cultural and societal systems in which we exist.
British physicist, Dr. Jess Wade, was reminded of this when she created a biography for prominent climate scientist Dr. Kim Cobb, discovering that deserving women like Cobb whose names — and lengthy list of achievements — had not been curated Wikipedia, the go-to site for most folks seeking information on the Internet. Naturally, male scientists do not suffer from the same issues and are often credited for achievements at the expense of female colleagues.
Google Dr. Rosalind Franklin and find out how bigot and all-around horrible human being James Watson stole her data and got credit for “discovering” DNA. He’s so bad he was stripped of honorifics after making bigoted comments about race and intelligence. Look up Dr. Arthur Eichengrün and find out how the precursor to the company Bayer, who collaborated with Nazis, gave credit for the discovery of aspirin to Dr. Eichengrün’s non-Jewish technician because of anti-Semitism and STILL haven’t acknowledged Eichengrün’s contribution. Yuck. I was today years old when I learned about Dr. Sophia B. Jones, the first Black female graduate of the University of Michigan’s Medical School in 1885 and later became the first female faculty member at Spelman College and spearheaded public health programs and health equity initiatives for Black Americans. There are countless other stories we’ve never heard of because of white supremacy and patriarchy, which celebrates the achievements of straight cis white males and minimizes or erases all others.
Dr. Wade decided to address this disparity by writing over 1,750 Wikipedia pages for female and minority scientists who didn’t already have their accomplishments documented on the site. Check out her own Wiki page, too! Not all heroes wear capes – some wear lab coats and cool glasses.
I’m totally going to make a Wikipedia page for myself. Men do it all the time, so why not??
Shout out to Dr. Wade, to the people behind these stories and their amazing contributions to science, and to a future in which we trade bias and bigotry for inclusiveness and giving credit where credit is due to everyone!
Thanks to my gal pal Florence Cardon for sharing the Washington Post article link with me, and to TikTok creator @inevitablebetrayal for shining a light on Bayer.
It’s Day 16 of National Breast Cancer Awareness Month! Today’s topic will cover one of the oldest targeted breast cancer drugs developed that is still used in the clinic today—tamoxifen. I’ve been taking it for 3 1/2 years, and millions of other breast cancer survivors with ER+ breast cancer have taken this drug as part of their treatments to prevent recurrence. But how was it discovered? How does it work?
Like many scientific discoveries, the discovery of tamoxifen was an accident. ICI46,474, later named tamoxifen, was first synthesized in 1966 by scientists working for a company that would become AstraZeneca. The goal of the project was to find a new chemical compound that could be made into a birth control drug. Laboratory studies were promising, but they found it didn’t work as a form of contraception in humans. This could have been the end of the story for tamoxifen, but one of the members of the team thought it might work as a breast cancer drug. In 1971, tamoxifen was tested in a clinical trial conducted in the UK on “late or recurrent carcinoma of the breast.” Thankfully, it worked!
How does it work? Since it started out as a candidate contraceptive, it makes sense that it was designed to block estrogen, a female hormone that helps prepare the uterus and uterine lining for pregnancy. It is in a class of drugs known as Selective Estrogen Receptor Modulators (SERMs), which are compounds that compete with the hormone estrogen for binding to its receptor. Normally, when estrogen binds to its receptor in the body, it triggers processes in the cell that make it divide, or produce more cells. This is called proliferation. In cancers with too many estrogen receptors (ER), estrogen in the body makes these cells grow uncontrollably. By binding to estrogen receptors in breast cancer cells, tamoxifen blocks this action and stops breast cancer cells from growing.
Around 70-80% of breast cancers are ER+, meaning that abnormal estrogen receptor activation is a key driver for growth of the breast cancer cells. Tamoxifen was a game changer for women with ER+ disease, reducing the annual breast cancer death rate by 31%. There are other drugs on the market that also block the activity of estrogen or downstream molecules in the estrogen receptor pathway, but tamoxifen remains standard of care for many cases of ER+ breast cancer.
As with any medication, tamoxifen comes with side effects that include: hot flashes, vaginal discharge, nausea, mood swings, fatigue, depression, hair thinning, constipation, loss of libido, dry skin. I experienced hot flashes, vaginal dryness and libido issues, and hair thinning, but they were not as severe as those I experienced with other estrogen blockers (aromatase inhibitors). For me, tamoxifen is a better balance between protection from recurrence and quality of life, but everyone’s physiology and experiences are different.
Be sure to talk to your healthcare providers about any side effects you experience. You don’t have to suffer in silence, and there are options to reduce side effects and improve your quality of life.
While most breast cancers are sporadic, meaning there’s no genetic predisposition (i.e. gene variant inherited from one or both of your parents that increases your risk of breast cancer) that caused the cancer, around 5-10% of breast cancers are thought to be familial. Knowledge is power, and knowing if you have a genetic risk for breast cancer can empower you to take charge of your health by surveillance and managing your risk.
How do inherited gene variants increase a person’s risk for breast cancer? Everyone has two copies of genes that we inherit from our parents. These genes have many different variants in the human population, and some specific gene variants are associated with increased risk of breast cancer. For example, inherited mutations in BRCA genes that make the gene product non-functional (i.e. no longer able to repair damage to DNA) increase the risk for breast and other cancers because the loss-of-function allows other mutations to build up in affected cells, which can eventually transform them into cancer cells. If you carry BRCA variants associated with cancer, you may be at greater risk and you can also pass these risk genes to your children.
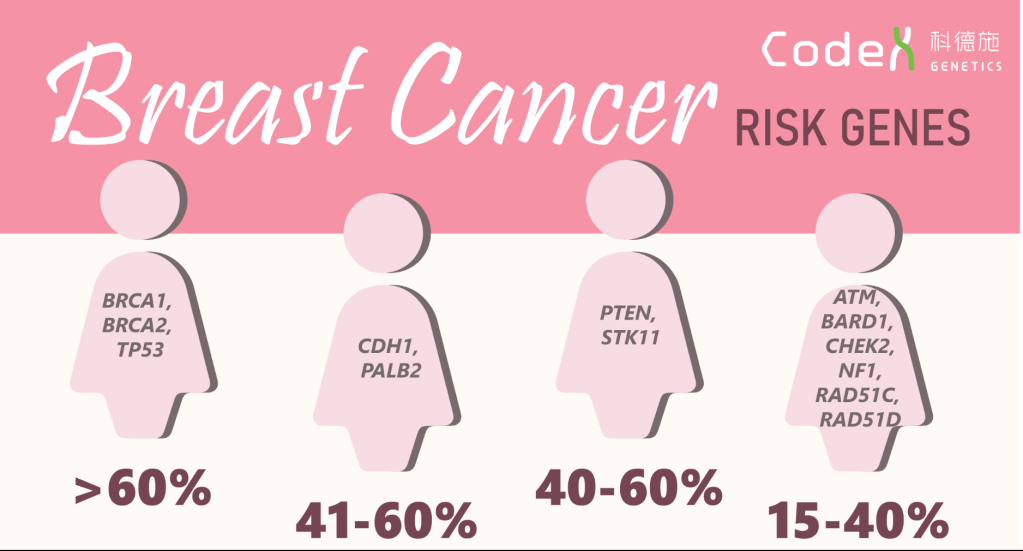
In addition to BRCA1 and 2 genes, other inherited gene variants have been identified that are associated with increased risk for breast cancer, as shown in the graphic below. Some of these genes, like TP53, PTEN, STK11, CHEK2, NF1, produce proteins that are also involved in regulating cell growth, so non-functional variants cannot put the breaks on cell growth and can cause cancer cells to grow uncontrollably. The PALB2, BARD1,ATM, and RAD51D gene products work like BRCA gene products to repair DNA damage, so loss of function increases the chance of accumulating mutations in cells, which can lead to cancer. The RAD51C gene product is involved in stopping cells with DNA damage from growing, so loss of function allows cells with mutations to divide and accumulate more mutations, which can lead to cancer.
Image Source Here. Percentages represent relative risk of breast cancer for people who have these gene variants associated with breast cancer.
Should you get genetic counseling and genetic testing? That’s a personal decision, but here are some recommendations from the CDC that might help you make your decision:
A strong family history of breast and ovarian cancer,
A moderate family health history of breast and ovarian cancer and are of Ashkenazi Jewish or Eastern European ancestry.
A personal history of breast cancer and meet certain criteria (related to age of diagnosis, type of cancer, presence of certain other cancers or cancer in both breasts, ancestry, and family health history).
A personal history of ovarian, fallopian tube, or primary peritoneal cancer.
A known BRCA1, BRCA2, or other inherited mutation in your family.
Knowing your risk can help you and your healthcare providers make decisions about surveillance and possible interventions. Take care of yourself, and if you can, find out about your family history of breast cancer.
It’s day 8 of National Breast Cancer Awareness Month! Breast cancer is widely considered to be a disease of biological females (e.g. cis women, intersex people), though cis men, trans men who forgo top surgery and trans women can develop breast cancer, as can non-binary, gender fluid, and literally any human being. That’s because we all are born with a small amount of breast epithelial tissue—cells in the breast that can grow, develop, and eventually produce and deliver milk to nursing infants.
Weird quirk of biology, but that’s how it goes. We all have a little breast tissue (unless we get it removed), so we can all theoretically get breast cancer. In the figures below, you can see a schematic of how epithelial tissue appears at birth and how it grows in response to hormone signals during puberty, as well as how the network of epithelial tissue from a mouse actually looks under a microscope. For more on how the process works, see my previous post on breast anatomy, structure, and function.
**Note – mice and other mammals have mammary epithelial tissue to make milk, which is one of the defining characteristics of a mammal, and the growth and development of mouse mammary epithelium is very similar to that in humans.**
During puberty, biological female breast epithelial tissue grows in response to female hormones like estrogen and progesterone. For biological males, the epithelium doesn’t grow in response to male hormones like testosterone, leaving only a small cluster of epithelium behind. Since biological females grow more epithelium and are exposed to hormones that make these cells grow, they have a greater risk for developing breast cancer. But biological males are still at risk, since the small amount of breast epithelium left behind after puberty can become cancerous.
How does this happen? First of all, the number one risk factor for cancer in general is age. See my previous blog posts, Intro to Cancer and Cancer 101, for how normal cells become cancer. CNN version – it involves random mutations in DNA that alter genes that tell cells to grow and/or in a small percentage of cases inherited gene variants like BRCA1 and BRCA2 (see previous post on how BRCA genes work). If enough of these mutations accumulate over time in a breast epithelial cell, that cell can transform into cancer.
While more rare in biological males, get enough mutations in a breast epithelial cells and you get male breast cancer. About 1 in every 100 breast cancer cases diagnosed in the United States is found in a man. According to the CDC, risk factors include: getting older, genetic mutations and a family history of breast cancer, previous radiation therapy in the chest area, hormone therapy treatment for prostate cancer, Klinefelter syndrome (in which a person has an extra X chromosome), some conditions that affect the testicles (like injury or removal), liver disease, being overweight, and being obese.
If you have a family history of breast cancer and ovarian cancer, consider genetic counseling and testing for BRCA1 and BRCA2 variants associated with increased risk of breast cancer. In men, mutations in these genes can increase the risk for breast cancer, prostate cancer, and pancreatic cancer (see CDC).
As with female breast cancer, early detection and diagnosis is key for a good prognosis. Pay attention to your body and any changes in your breast area, and look for symptoms including:
A lump or swelling in the breast. Redness or flaky skin in the breast. Irritation or dimpling of breast skin. Nipple discharge. Pulling in of the nipple or pain in the nipple area.
Also, don’t let stigma, shame, or toxic masculinity keep you from seeking help and advice from your healthcare provider. Since male breast cancer is rare, you may feel like you’re alone, but there are resources and survivor networks available to help, ones that are decidedly not pink and are tailored for men. Ask your healthcare provider about local and online support groups, mental health support, and other resources. For more information on male breast cancer, check out these resources: Breastcancer.org, The National Cancer Institute, The American Cancer Society, The National Breast Cancer Foundation, Susan G. Komen.
It’s day 6 of National Breast Cancer Awareness Month. I’m creating a new post every day in the Month of October to spread awareness, information, accessible science, practical advice, and humor. I can write about the science of breast cancer all day, and I’ve got plenty of stories to tell and woo woo bullshit to debunk, but I really want to hear from y’all.
What do you want to know about breast cancer, breast health, breast biology, treatments, surgeries, radiation, or any topic? Want me to investigate something a friend told you would help with your cancer, or some off the wall thing you found on FaceBook? Need resources on getting screening mammograms, including financial assistance, and on getting breast healthcare? Want to see pictures of my cats and hear about how they’ve kept me entertained and happy during my breast cancer years?
Let me know!
I’m a research whore – send me down a rabbit hole and help me find something new! Comment on this post with what you want to know and I’ll select three folks at random to receive a signed copy of Talking to My Tatas, my breast cancer book.
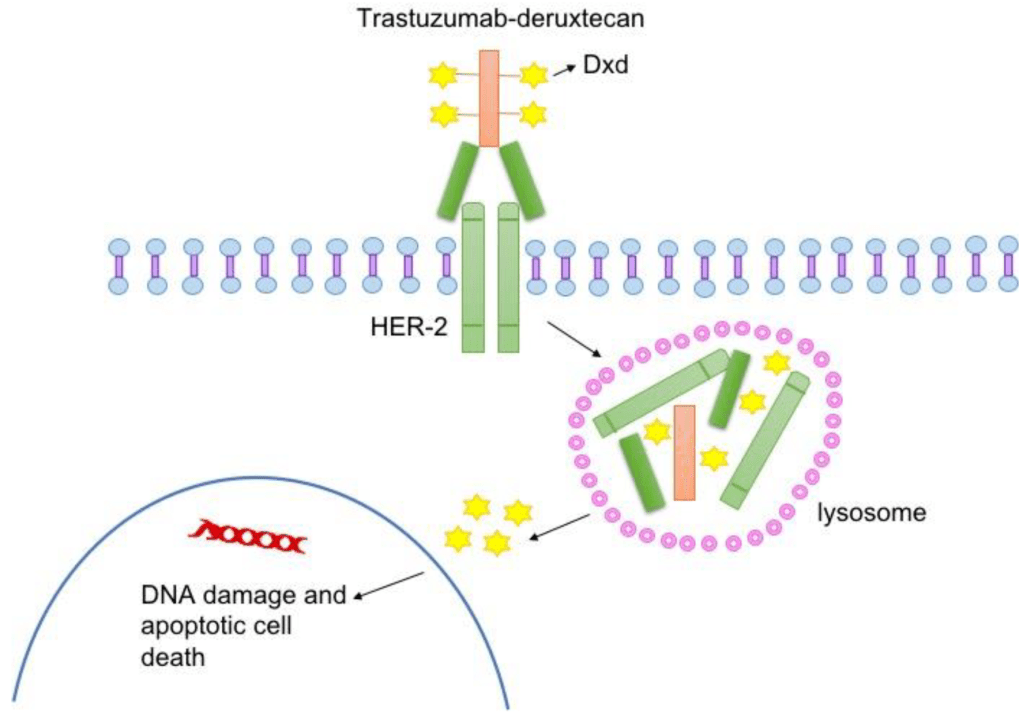
For today’s topic, let’s talk about the DESTINY-4 clinical trial that represents a HUGE advance in breast cancer treatment options for people with HER2-low advanced cancer. As I discussed in my previous post about breast cancer subtypes, HER2+ breast cancers are diagnosed based on how they look under the microscope and if they have extra copies of the gene that makes the HER2 cell surface receptor protein and/or if they express higher than normal levels of HER2, a protein that makes breast cancer cells grow uncontrollably.
The standard of care is to classify HER2+ breast cancers as meeting a threshold for HER2 receptor expression. Cancers that express levels of HER2 below that threshold were considered HER2-negative and not treated with HER2 targeted therapies. But people with low levels of HER2 in their breast tumor could still benefit from HER2-targeted therapies. To test that hypothesis, Dr. Shanu Modi, MD, of the Memorial Sloan Kettering Cancer Center led a clinical trial that tested an antibody drug conjugate called Trastuzumab Deruxtecan (T-DXd) to see if patients with HER2-low metastatic breast cancer benefitted from this treatment. This drug consists of trastuzumab, an antibody that binds to HER2 on tumor cells, and a toxic drug that is delivered directly to the tumor by trastuzumab, which kills cancer cells. People who received this drug in the trial lived longer and had a longer time before their cancer progressed compared to patients who received chemotherapy. The drug reduced tumor burden, the amount of cancer in the body. The major side effects of treatment with this drug include heart and lung function issues, which need to be closely monitored in people taking this drug.
Not only do these results provide hope and more treatment options for patients with metastatic breast cancer, they will likely change the way we classify breast cancers by molecular subtype, adding HER2-low to the classification system. Ongoing clinical trials will test this drug on patients with different levels of HER2 expression to determine the range of expression that defines HER2-low tumors likely to respond.
To learn more about Trastuzumab Deruxtecan, visit the National Cancer Institute website. Click here for more information about breast cancer treatment clinical trials.
It’s the fifth day of National Breast Cancer Awareness Month 2022! Quick update from yesterday – my (hopefully) last breast reconstruction procedure went great! I’m home recuperating and enjoying love from my fur babies and my family. I haven’t looked at the result yet, but the left side of my surgical bra looks fuller. Hooray!
Now, back to the subject of breast cancer molecular subtypes! To recap, breast cancer isn’t a single disease. It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
Molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment, include four subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer TNBC.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about the triple negative subtype, which do not express hormone receptors for estrogen and progesterone and also do not express express a cell surface protein receptor called HER2. That’s how it got its name, triple negative, because of the three receptors it does not express. These breast cancers have other ways of growing abnormally that don’t involve hormones or HER2, and they tend to grow very fast. For example, some TNBCs have higher higher than normal levels of EGFR receptors, which are in the same cell surface receptor family as HER2. Like HER2, EGFR normally tell breast cells to grow during normal development in puberty. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Aside from targeting EGFR, a strategy being tested in clinical trials, people with TNBC have fewer treatment options with targeted therapies (therapies that inhibit hormone receptors and HER2) than other subtypes.
Aside from EGFR receptors, what make TNBC cells grow? There are several molecular pathways that become altered in TNBC. These pathways often function in normal breast epithelial cells telling them to grow when appropriate (cell surface receptors like EGFR, FGFR, and CSF1-R). When receptors on the surface of the cell becomes activated, they send signals to the breast cell that tells it to grow, like when your breasts are growing during puberty. Normally, after puberty, the receptor and related receptors are no longer activated and your breast cells stop growing. In breast cancer, your breast cells make too many receptors, which become constantly activated, making your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these receptors make the cancer cells grow uncontrollably.
One interesting characteristic of TNBC is that this subtype often has more interactions with the body’s immune system, meaning that immune cells travel to the tumor, get inside of it, and try to kill cancer cells and eliminate them from the body. Many cancer cells develop defenses against the immune system, using cell surface proteins like PD-1, PD-L1, and CTLA4 to shut down the immune cells. Tumors with lots of immune cells, called immunologically “hot,” may respond well to immune therapies that block the activity of PD-1, PD-L1, and CTLA4. The drug Pembrolizumab, which targets PD-1, is used to treat advanced TNBC. The drug Sacitiuzumab Govitecin was recently approved to treat TNBC. More on that below!
TNBC breast cancer is not as common as HR+ breast cancer, accounting for 15-20% of breast cancers. However, these breast cancers are often more aggressive and faster growing than HR+ breast cancer. They also disproportionately affect younger women and women of African descent. They are diagnosed by a pathologist based on analysis of gene and protein expression if ER, PR, and HER2 present in cancer cells in a biopsy and in the tumor after surgical removal. Low or no expression of these three receptors leads to a diagnosis of TNBC. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor.
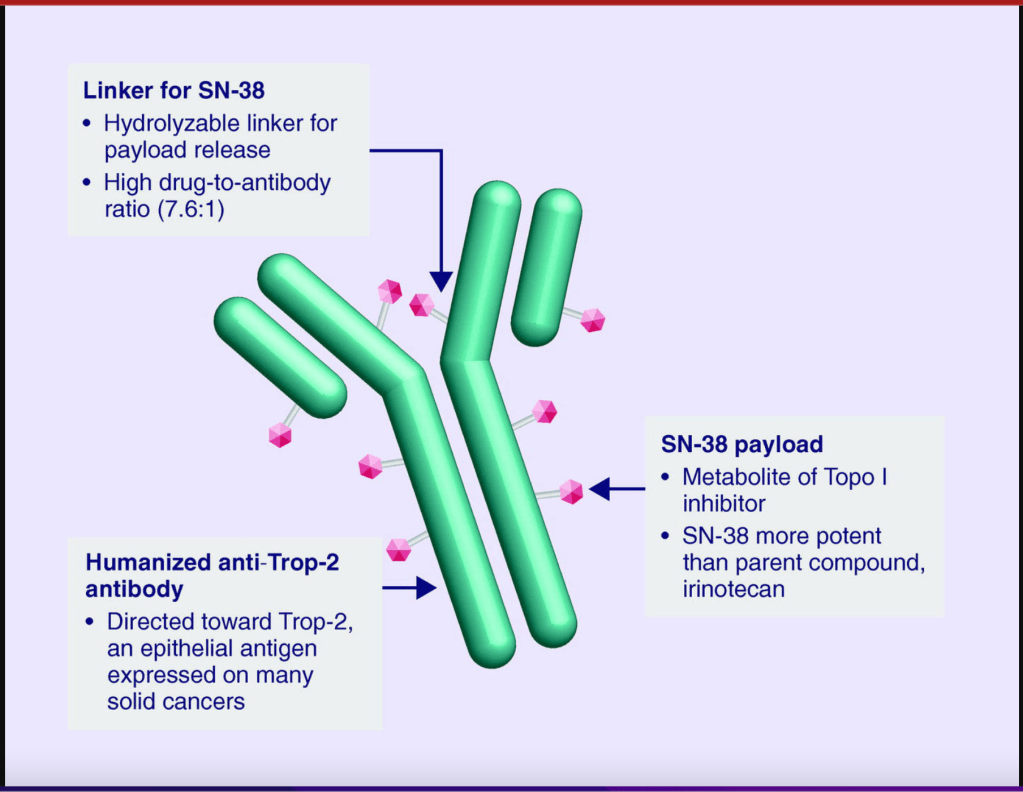
Follow-up treatments include chemotherapy, which was the only option for people diagnosed with TNBC for many decades. Recently, drugs developed specifically to treat TNBC have been approved and are being used in the clinic and undergoing additional testing in clinical trials to refine and optimize their ability to work with other drugs to kill more cancer cells. I discussed Pembrolizumab above. Let’s go over a little bit about Sacituzumab Govitecan. This drug binds to the cell surface protein Trop-2. Many TNBCs have higher than normal levels of Trop-2 on the surface of their cells. Sacituzumab Govitecan, approved in April of 2022, as a treatment for metastatic TNBC, is an antibody-drug conjugate that uses the an antibody against Trop-2 to carry a toxic drug directly to breast cancer cells with high levels ofTrop-2, targeting tumor cells and reducing damage to normal cells and tissues.
These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on TNBC, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams. Though TNBC is trickier to detect, screening mammography remains a vital tool for early detection of TNBC and other breast cancer cell types.
It’s the third day of National Breast Cancer Awareness Month 2022! To recap, breast cancer isn’t a single disease. It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
Molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment, include four subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about the HER2-enriched (also called HER2+) subtypes, which express a cell surface protein receptor called HER2. These breast cancers have higher than normal levels of HER2 receptors, which normally tell breast cells to grow during normal development in puberty. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Luminal B breast cancers have too much of the cell surface receptor HER2 in addition to having too much estrogen and progesterone receptors (ER/PR +ve), as do breast cancers that do not also express hormone receptors (HER2-enriched).
How does HER2 receptors make breast cancer cells grow? When the receptor on the surface of the cell becomes activated, it sends a signal to the cell that tells it to grow, like when your breasts are growing during puberty. Normally, after puberty, the receptor and related receptors are no longer activated and your breast cells stop growing. In breast cancer, your breast cells make too many HER2 receptors, becoming constantly activated ,making your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these HER2 receptors make the cancer cells grow uncontrollably.
HER2+ breast cancer is not as common as HR+ breast cancer, accounting for 10-20% of breast cancers. However, these breast cancers are often more aggressive and faster growing than HR+ breast cancer. They are diagnosed by a pathologist based on analysis of HER2 gene expression and HER2 proteins present in cancer cells in a biopsy and in the tumor after surgical removal. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor. .
Follow-up treatments include chemotherapy andHER2-targeted therapies that block the activity of HER2 on breast cancer cells, including antibody drugs that bind to HER2 receptors and cause them to be degraded by the cell as well as triggering the body’s natural immune system to attack HER2+ tumor cells. These drugs include Trastuzumab and Pertuzumab. A derivative of Trastuzumab called Ado-trastuzumab emtansine (also called T-DM1) is an antibody-drug conjugate that uses the Trastuzumab antibody to carry emtansine chemotherapy directly to breast cancer cells with high levels of HER2, targeting tumor cells and reducing damage to normal cells and tissues.
These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on HER2+ positive breast cancer, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams.
It’s the second day of National Breast Cancer Awareness Month 2022! Did you know that breast cancer isn’t a single disease? It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
This post and upcoming posts will focus on molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment. There are currently four molecular breast cancer subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about Luminal A and Luminal B subtypes, which are hormone receptor-dependent (hormone receptor-positive, also known as estrogen receptor-positive or estrogen receptor/progesterone receptor-positive). These breast cancers have higher than normal levels of receptors for estrogen (ER+) and progesterone (PR+), which normally tell breast cells to grow during pregnancy as they get ready to start producing milk. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Luminal B breast cancers also have too much of the cell surface receptor HER2, which also makes breast cells grow uncontrollably, contributing to cancer. HER2 positive breast cancer will be covered in the next post.
How do estrogen and progesterone receptors make cancer cells grow? Estrogen produced by your body binds to molecules called receptors. When estrogen or progesterone enters a breast cell, it binds to a partner, called a receptor. When the receptor binds to the hormone, it sends a signal to the cell that tells it to grow, like when you’re pregnant and your breasts are getting ready to make milk for when the baby is born. Normally, after pregnancy and lactation, estrogen levels in your body go down and your breast cells stop growing. In breast cancer, your breast cells make too many receptors, so when estrogen levels go up in your body, like during your normal menstrual cycle, your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these estrogen and progesterone receptors make the cancer cells grow uncontrollably.
Hormone receptor positive, also referred to as ER+, ER/PR+ breast cancer, is the most common type of breast cancer, accounting for 70-80% of breast cancers. They are diagnosed by a pathologist based on analysis of hormone receptor proteins present in cancer cells in a biopsy and in the tumor after surgical removal. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor. Depending on stage and grade, the ER/PR+ breast cancers should be analyzed by tumor genomic tests like Oncotype Dx or MammaPrint, which helps predict how likely the cancer is to recur (i.e. come back) and if chemotherapy is necessary for treatment.
Follow-up treatments include hormone therapies that block the activity of estrogen in the body, like the drug Tamoxifen, drugs that block estrogen production by the body, aromatase inhibitors like Letrozole, Arimidex, and Exemestane, or drugs that degrade estrogen receptor like Fulvestrant. Other ER+ breast cancer treatments include drugs that block the activity of proteins that drive cell growth (CDK inhibitors), including Ribociclib, Palbociclib, and Abemaciclib. These are typically used in combination with endocrine therapies like Tamoxifen/AIs/Fulvestrant to treat metastatic breast cancer, which has spread to other parts of the body. For women diagnosed with cancer who haven’t yet undergone menopause, medically induced menopause may be recommended. These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on hormone receptor positive breast cancer, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams.