Use the promo code 22JOYSALE at checkout to get the sale price now through January 6, 2023!
This is a great deal, as you’ll save over $12 on the Hardback and almost $12 on the eBook. Know someone who is going through breast cancer? This would be a helpful gift. Know someone who’s a science loving nerd? They’ll probably like it, too!
It’s day 26 of National Breast Cancer Awareness month! Today, I had the opportunity to appear on the Tampa Reads segment of Fox 13 in Tampa with anchor Linda Hurtado! I was able to share my breast cancer story with a bit about science, about my personal story, and a bit about Talking to My Tatas.
It was a great experience and I hope I convinced some viewers to schedule their mammograms! Shout out to Linda Hurtado, Lisa Emerson, and the rest of Fox 13 News Team!
It’s day 23 of National Breast Cancer Awareness Month! I skipped a few days due to lack of spoons (see my previous post about spoon theory and chronic illness), but I have some extras today and am excited at the prospect of bringing my message to folks in Tampa, Florida, and beyond!
My amazing Literary Agent, Barbara Rosenberg, put me in touch with Linda Hurtado, an award-winning news anchor by day who writes heart stopping thrillers as Linda Bond (and I totally recommend checking out her books!). Linda then invited me to appear on her live show for Breast Cancer Awareness Month! It’s scheduled for Wednesday, October 26, at 12:00 pm EST for her Tampa Bay Reads segment. I’ll be talking about breast cancer from both a patient and research perspective, talking about the book, and hopefully convincing viewers to schedule their mammograms!
This will be my first television appearance and I’m both excited and a little nervous, but I have faith in Linda and I’ll just be prepared to be poised but still be myself as I share my story and hopefully some more information about breast cancer that the public needs to know.
Super grateful for the opportunity and hope it helps me make a difference! Wish me luck!
I’ll be sure to post the link in a future blog post!
It’s day 6 of National Breast Cancer Awareness Month. I’m creating a new post every day in the Month of October to spread awareness, information, accessible science, practical advice, and humor. I can write about the science of breast cancer all day, and I’ve got plenty of stories to tell and woo woo bullshit to debunk, but I really want to hear from y’all.
What do you want to know about breast cancer, breast health, breast biology, treatments, surgeries, radiation, or any topic? Want me to investigate something a friend told you would help with your cancer, or some off the wall thing you found on FaceBook? Need resources on getting screening mammograms, including financial assistance, and on getting breast healthcare? Want to see pictures of my cats and hear about how they’ve kept me entertained and happy during my breast cancer years?
Let me know!
I’m a research whore – send me down a rabbit hole and help me find something new! Comment on this post with what you want to know and I’ll select three folks at random to receive a signed copy of Talking to My Tatas, my breast cancer book.
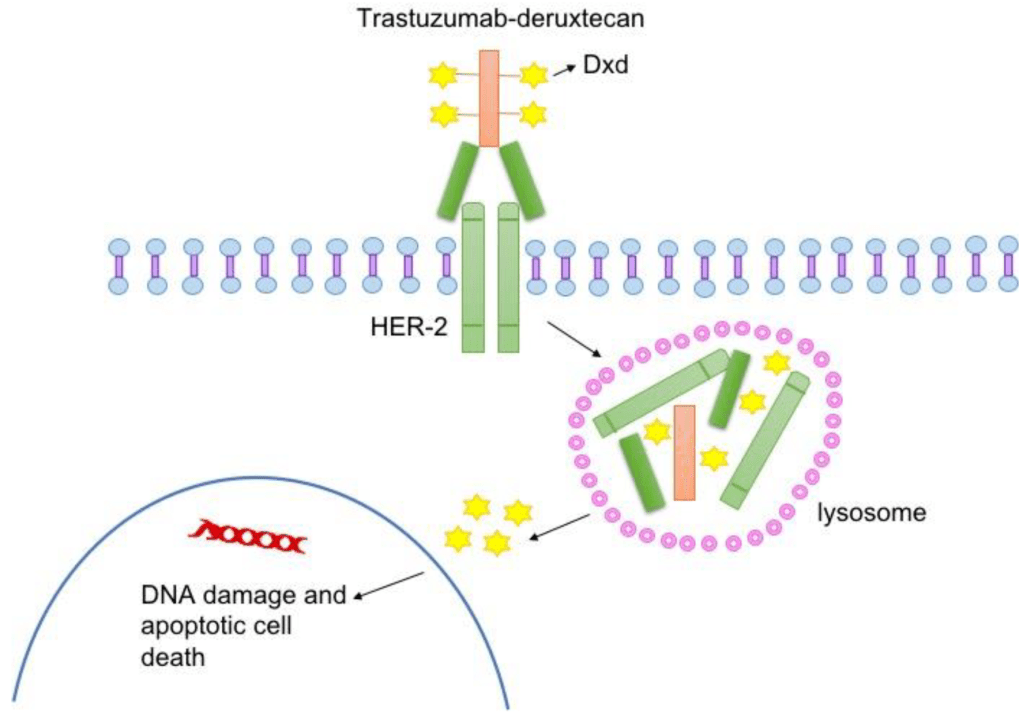
For today’s topic, let’s talk about the DESTINY-4 clinical trial that represents a HUGE advance in breast cancer treatment options for people with HER2-low advanced cancer. As I discussed in my previous post about breast cancer subtypes, HER2+ breast cancers are diagnosed based on how they look under the microscope and if they have extra copies of the gene that makes the HER2 cell surface receptor protein and/or if they express higher than normal levels of HER2, a protein that makes breast cancer cells grow uncontrollably.
The standard of care is to classify HER2+ breast cancers as meeting a threshold for HER2 receptor expression. Cancers that express levels of HER2 below that threshold were considered HER2-negative and not treated with HER2 targeted therapies. But people with low levels of HER2 in their breast tumor could still benefit from HER2-targeted therapies. To test that hypothesis, Dr. Shanu Modi, MD, of the Memorial Sloan Kettering Cancer Center led a clinical trial that tested an antibody drug conjugate called Trastuzumab Deruxtecan (T-DXd) to see if patients with HER2-low metastatic breast cancer benefitted from this treatment. This drug consists of trastuzumab, an antibody that binds to HER2 on tumor cells, and a toxic drug that is delivered directly to the tumor by trastuzumab, which kills cancer cells. People who received this drug in the trial lived longer and had a longer time before their cancer progressed compared to patients who received chemotherapy. The drug reduced tumor burden, the amount of cancer in the body. The major side effects of treatment with this drug include heart and lung function issues, which need to be closely monitored in people taking this drug.
Not only do these results provide hope and more treatment options for patients with metastatic breast cancer, they will likely change the way we classify breast cancers by molecular subtype, adding HER2-low to the classification system. Ongoing clinical trials will test this drug on patients with different levels of HER2 expression to determine the range of expression that defines HER2-low tumors likely to respond.
To learn more about Trastuzumab Deruxtecan, visit the National Cancer Institute website. Click here for more information about breast cancer treatment clinical trials.
One of the things I love about my work in advocacy is discovering amazing people who are doing the work and making a difference! Valeda Keys is one such remarkable person. She’s a Global Ambassador for Breast Cancer Awareness, using her platform and the Non-Profit organization she founded, Valeda’s Hope, to assist women in their journey from diagnosis to remission. She has one hell of a compelling story that includes a family history of breast cancer, a personal battle with breast cancer that included seven surgeries, and finding strength and empowerment in helping others.
When I learned about her work on LinkedIn, I was blown away.
Valeda, who is an Author, Speaker, LPN, Non-Profit Founder, Breast Health Navigator, and all around incredible human being, helped her mother through a breast cancer diagnosis, treatment, and later recurrence. A dream told her that she would one day endure her own battle with breast cancer, which unfortunately came true in 2010. Luckily, because of her family history, Valeda started receiving mammography screening at the age of 27 and kept up with her screenings, which allowed her healthcare team to detect her first breast cancer at an early stage. After a lumpectomy, she received the results of her genetic testing, which revealed that she carries a variant of theBRCA-2(BReast CAncer gene 2) gene associated with an increased risk of breast and ovarian cancer.
Everyone has two BRCA1 and two BRCA2 genes, but sometimes a variant of one of these genes that doesn’t work gets passed down from one of your parents. If something happens to the other copy of the BRCA gene in a cell (for example, a cell from your breast or ovary), it can increase your risk for cancer. Why? BRCA genes encode information to make proteins that help fix damage to DNA. DNA molecules encode and store all the information a cell needs to make proteins, which allows a cell to live and perform its function. When DNA is damaged, it messes with the code, and if the damage isn’t repaired, cells make defective proteins that don’t function well or in the case of cancer-causing oncogenes, function too well. Defects in some genes make cells grow uncontrollably, and sometimes those cells turn into cancer cells. Variants of BRCA genes that don’t function to fix DNA damage makes it more likely for oncogenes to get activated and make cells grow uncontrollably, leading to cancer. In the graphic above, you can see a DNA repair deficient breast cell in which the BRCA genes encode DNA repair proteins that don’t work. Because the defective BRCA gene produces a defective protein, the cell can’t repair DNA damage and gets a lot more mutations in a lot of different genes. Some of these mutations create defective proteins that let the cell grow uncontrollably, even without estrogen (E2) or other cues from the body that tell cells when to grow. See my Cancer 101 blog post and my other blog poston how cells become cancerous for a refresher on the cell biology of breast cancer, DNA damage and how it leads to cancer, and oncogenes.
End Science Break
Now, back to Valeda’s story. Since she carries a variant of BRCA-2 that doesn’t work, she was still at risk for getting another breast cancer or ovarian cancer after her first breast cancer diagnosis. She decided to keep her breasts and get screened more often, a valid choice. (Note: there are no right or wrong choices when it comes to keeping your breasts or having a double mastectomy. There are only informed choices you make with your healthcare team that are right for you.). She also endured radiation therapy that led to some serious complications, and was treated with tamoxifen, a drug that blocks estrogen function. In spite of this, she was diagnosed with a new breast cancer in 2011 and opted for a double mastectomy and autologous reconstruction (i.e. reconstruction using her own tissue from her abdomen to build new breasts), which unfortunately came with some complications, and later had a hysterectomy.
Through it all, she remained focused and determined not to let breast cancer get in the way of living a full life and achieving her goals. Her faith helped her through, and it gave her a mission to educate, empower, and help other women through their own breast cancer journeys. Among the many amazing things she does through Valeda’s Hope, Valeda sponsors a ton of mobile mammography events and encourages women to keep up with life-saving screenings. She shares her knowledge and experience through speaking engagements and educational events like Valeda’s Hope Pink & Pearls Luncheons. Valeda also hosts events that provide emotional and physical support as well as information about genetic testing for breast cancer risk genes, and so much more.
A fantastic book by an amazing survivor!
I’ve said it before, and I’ll say it again: the breast cancer survivor community is so supportive! Survivors support other survivors, patients, and caregivers. As a survivor, Valeda is using her voice and actions to help other women survive and thrive, and that deserves a spotlight, kudos, and celebration!
The book has been out for about 3 weeks and I’ve been thrilled/nervous/pee-my-pants-excited to see my Amazon ranking as well as checking for ratings and reviews on Amazon, Goodreads, and other retail sites like Barnes & Noble, Walmart, Google Books, and Rowman & Littlefield!
For a brief, beautiful, shining moment, it was the #1 New Release in Breast Cancer and Oncology on Amazon, and I have the screenshots to commemorate it!
Pics or it didn’t happen!
Want a sneak peek? Of course you do! Here’s an excerpt from Chapter 16 that deals with an exciting new development in cancer research and treatment – harnessing the patient’s own immune system to seek out and destroy cancer cells through immune checkpoint inhibitors.
EXCERPT
I’ll also take comfort in the fact that we’re getting new weapons in the arsenal for fighting breast cancer. Antitumor immunity is the hottest thing to hit the field of cancer research since the 2001 approval of Gleevec (a game-changer drug used to treat chronic myelogenous leukemia that targets the oncoprotein product of the Philadelphia chromosome that drives the disease) and the 2006 approval of Gardasil (first vaccine targeting the human papilloma virus strains that cause most cervical cancers). Recently Frontiers in Immunology published the history of antitumor immunity efforts leading to the development of immune-checkpoint inhibitors available in the clinic today, the use of engineered T-cells taken from patients and altered to fight their cancer, and oncolytic viruses.2 I’ll go over the basics, including how antitumor immunity works and the challenges we still face in getting tumors to respond.
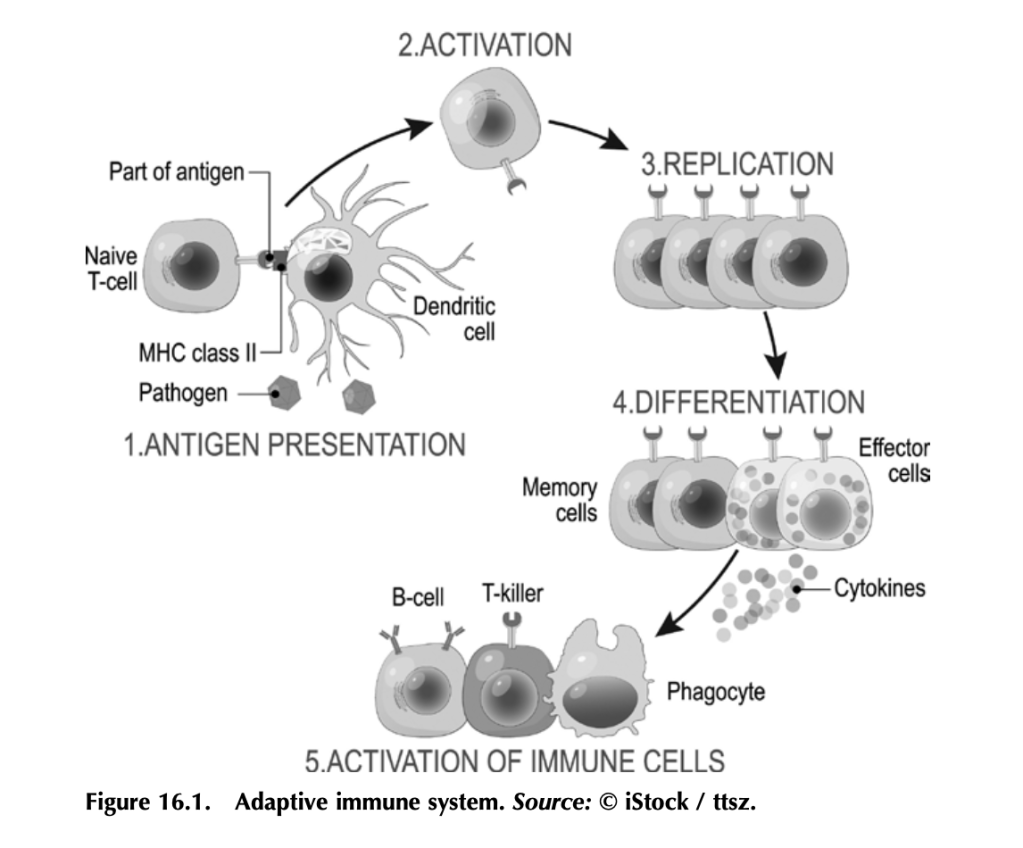
Before we get into how antitumor immunity works, we need to understand how the immune system works to fight infection. It’s a complex beast, but here are some basics. Your immune system functions to mount a rapid and robust defense when your body encounters a pathogen (e.g., a virus or bacteria that causes disease) in your daily life. The arm of the immune system that does this is called the adaptive immune system (figure 16.1). The other arm is the innate immune system, which includes natural barriers like skin, the tiny hairs and mucous in your nose, and stomach acid. The adaptive immune system is what antitumor immunity treatments harness. It is also altered by tumors to suppress tumor immune responses and exploited to work for the tumor. (More on that in a bit.)
The adaptive immune system works like this: Specialized cells identify a potential threat (e.g., an infection), and they carry information about that threat in the form of bits of protein called antigens to other immune cells. If the threat is credible, those immune cells get activated and fight the threat. First the specialized cells that identify a potential threat patrol your body, looking for something suspicious. Cells like macrophages and dendritic cells, which roam around various organs and tissues, find pathogens (a bacteria, virus, or other microbe that causes disease) or unhealthy cells infected by pathogens, and eat them (the fancy term is phagocytosis). Infected or damaged cells send out protein signals called cytokines as a distress call to attract these patrolling macrophages and dendritic cells. While “digesting” the bacteria or infected cell, macrophages and dendritic cells salvage proteins or pieces of proteins—antigens—that identify the bacteria or virus as “other,” and they present these to immune cells, usually in lymph nodes, which in turn mount an immune response. Macrophages and dendritic cells are known as professional antigen presenting cells (APCs).
When activated by APCs, immune cells called B-cells produce antibodies against the antigen, which can do a lot of things to fight an infection. Some antibodies neutralize the pathogen by binding it and stopping it from entering a cell. Other antibodies tag infected cells as a signal for other immune cells to come and kill them. Others coat pathogens or infected cells in a process called opsonization (meaning “the process of making tasty”), which signals other cells like macrophages to come and eat the coated pathogens or cells. Specialized B-cells called memory B-cells store the information about the antigen so your immune system can recognize the pathogen when it hits you again and mount a faster immune response.
Other immune cells called T-cells, which are particularly relevant to antitumor immunity, become activated by APCs and mount a different kind of immune response. Cytotoxic T-cells seek out and kill infected or damaged cells, and helper T-cells help activate B-cells so they make antibodies, activate cytotoxic T-cells, and activate macrophages to go eat nasty invaders and infected cells. Memory T-cells also store information about past infections to mount a rapid, strong response the next time your body sees it.
That’s a simplified but hopefully digestible explanation of immunity and the major players (there are other immune cells, but APCs, B-cells, and T-cells are the biggies).
Memory is key to protection, and memory is built by exposure to pathogens.
Put a pin in that concept for when we get to anticancer vaccines, and also remember what T-cells do for when we get to engineered CAR T-cells and oncolytic viruses.
Working out how to harness your body’s own immune system to fight cancer isn’t a new idea. It’s been under investigation since the nineteenth century. In fact, in chapter 5 we covered the way trastuzumab (trade name Herceptin), a humanized anti-HER2 antibody, targets HER2-expressing breast cancer cells for death. Herceptin and other monoclonal antibodies mimic the natural activity of antibody- producing B-cells to deliver therapies and tag cancer antigen–expressing cells for immune-mediated destruction. But it was the discovery of checkpoint inhibitors—proteins that put T-cells in a state of exhaustion and inactivity in pathways that are exploited by many cancers— that led to the first molecularly targeted therapies designed to boost antitumor immunity. Doctors James Allison and Tasuku Honjo pioneered this Nobel Prize–winning work.3
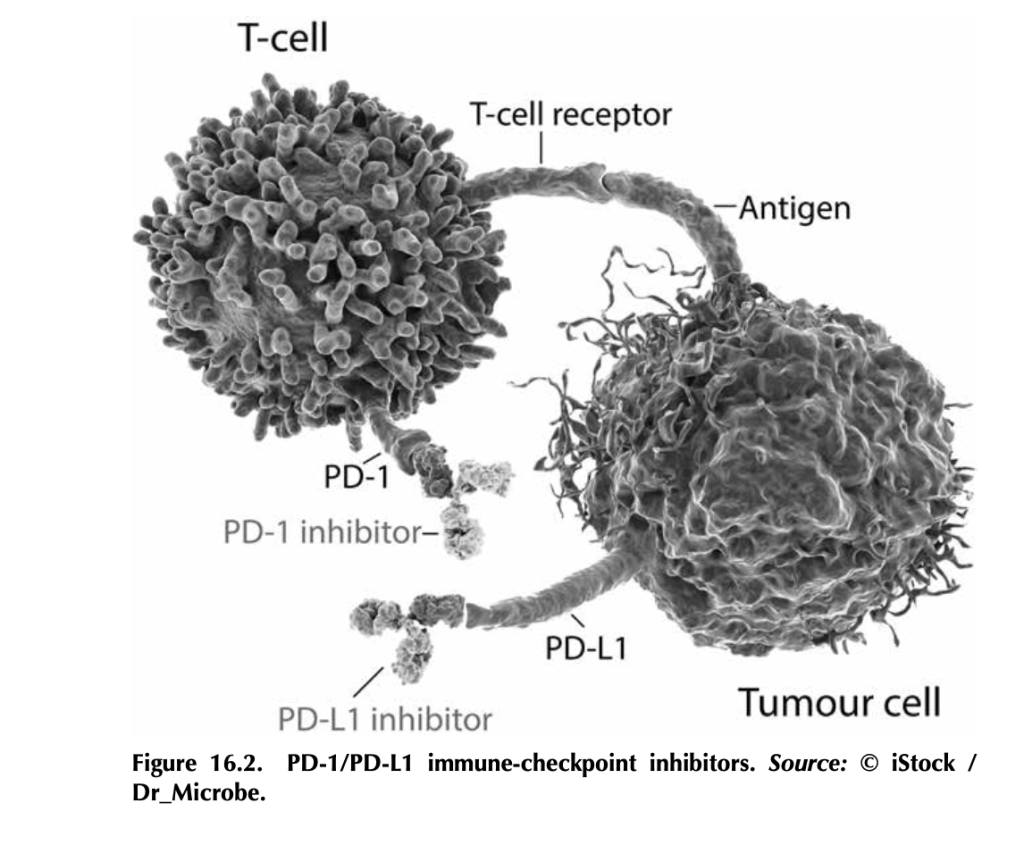
What are immune-checkpoint inhibitors, and how do they work? T- cells, particularly cytotoxic T-cells that actively kill their targets, bind to antigens on tumor cells through their T-cell receptors. But tumor cells, being the adaptable beasts that they are, can produce proteins like PD-L1 (programmed death ligand 1), which bind to PD-1 (programmed cell death protein 1), proteins on T-cells. This interaction tells the T- cell to stand down by tricking it into thinking that the tumor cell is “self” and should be protected. Signaling networks like this normally promote self-tolerance so that your immune system doesn’t attack your own healthy cells (figure 16.2). In tumors, it works by telling tumor- infiltrating T-cells, if present, to go into a state of inactivity. Drugs that target PD-L1—like atezolizumab (trade name Tecentriq), durvalumab (trade name Imfinzi), and avelumab (trade name Bavencio)—and drugs that target PD-1—like nivolumab (trade name Opdivo) and pembrozolimuab (trade name Keytruda)—are FDA-approved mono- clonal-antibody therapies that block interactions between PD-1/PD-L1 to unleash an antitumor immune response.4
Other immune-checkpoint molecules exploited by cancers include cytotoxic T lymphocyte antigen 4 (CTLA-4), the target of the first FDA-approved immune-checkpoint inhibitor ipilimumab (trade name Yervoy). Approved in 2011 for advanced melanoma, this drug had remarkable results. In fact, over 20 percent of the patients enrolled in the initial ipilimumab clinical trials (before the 2011 approval) are still alive and show no evidence of disease (NED).
There’s some incredible potential in targeting checkpoint inhibitors.
CTLA-4 is part of a cellular-signaling pathway that normally fine- tunes immune responses. CTLA-4 and a similar receptor, CD28, are expressed on two different T-cell types: (1) CD4+ helper T-cells, which help activate other immune cells to mediate adaptive immune responses, and (2) CD8+ cytotoxic T-cells, those cells that kill infected cells, damaged cells, and, if properly activated, tumor cells. Antigen- presenting cells make a protein called B7, which can bind to either CD28 or CTLA-4 on T-cells, and the effects on T-cell function are very different depending on what B7 binds. If it binds to CD28, B7 activates T-cell responses as a part of a complex of proteins that includes the T-cell receptor. Binding of B7 to CTLA-4 shuts down T- cell functions. CTLA-4 probably serves as protection from self-antigen recognition by inducing immune suppression, since laboratory mouse models engineered to not express CTLA-4 die from autoimmunity. This is the aspect of CTLA-4 function that gets highjacked by tumor cells. Drugs like ipilimumab block the suppressive activity of CTLA-4, which can allow T-cells to attack tumor cells.5
Here’s the kicker: The tumor actually has to have infiltrating T-cells for this to work, and not all tumors do. Tumors with T-cells that can be activated to fight the tumor are called “hot,” whereas tumors without T-cells are “cold.” One of the most aggressively researched topics in tumor immunology right now is how to make a cold tumor hot and thus responsive to antitumor immune therapies.
This is especially important for breast cancer, since most subtypes produce cold tumors. Right now, immune-checkpoint therapies are only approved for advanced triple-negative breast cancers that make the PD-L1 protein. Not all triple-negative breast cancers make PD-L1. Ongoing research is looking to expand the use of immune therapy in inflammatory breast cancer and the HER2+ subtype.6 Hopefully, with more research, we’ll figure out how to make more tumors responsive to immune therapy by making them hot (full of T-cells) and by discover- ing other immune checkpoints that can be targeted.
3. Heidi Ledford, Holly Else, and Matthew Warren, “Cancer Immunologists Scoop Medicine Nobel Prize,” Nature, October 1, 2018, https://www.nature. com/articles/d41586-018-06751-0.
4. See American Cancer Society medical and editorial content team, “Immunotherapy for Breast Cancer,” Treating Breast Cancer, American Cancer Society, Cancer.org, last revised December 3, 2020, https://www.cancer.org/ cancer/breast-cancer/treatment/immunotherapy.html.
6. Devon Carter, “Does Immunotherapy Treat Breast Cancer?” MD Anderson Center (website), University of Texas, March 26, 2021, https://www .mdanderson.org/cancerwise/does-immunotherapy-treat-breast-cancer.h00 -159385101.html.
Sometimes, if you’re lucky, something comes into your life just when you need it the most. That was my introduction to The Bloggess (aka Jenny Lawson aka Amazing/Funny/Fabulous human being). I LOVED her first book, Let’s Pretend This Never Happened (A Mostly True Memoir), gifted to me by my BFF. If you haven’t read it, treat yourself. Her other books are just as poignant, engaging, and hilarious. They’re like Pokemon – gotta catch them all! Or maybe potato chips – betcha can’t read just one. Something like that.
Better yet, grab the Audiobook! Jenny narrates it, and the humor and heartache and hope just flows from her voice directly to your brain cells, releasing serotonin and making you feel better no matter what you’re going through. Which brings me back to my first point – the something-that-comes-into-your-life-just-when-you-need-it-the-most point:
Shout out to @TheBloggess for keeping me company (via audiobook) through two breast biopsies today. You be funny! And awesome!
— Dana Brantley-Sieders, Ph.D. (@DBSieders) May 17, 2018
Yes, I am a fangirl and yes, I show love to show my appreciation!
The day I endured two breast biopsies was a bad day. It would have been worse without Jenny, who allowed me to escape into her world and kept me company while I was waiting to go on the slab. And guess what?
SHE FOLLOWED ME BACK ON TWITTER!!!!
This was the highlight of my year, people! It also kept me going and inspired me while writing Talking to My Tatas. Jenny’s story touched and inspired millions, and she’s saved lives, y’all! I wanted to do the same. Whenever I got frustrated, stuck, or wanted to just give up on the writing, querying, and rejections, I remembered Jenny.
Fast-forward to the present, and guess what? Jenny Lawson endorsed my book!
“I don’t know much about cancer, but I know good writing and humor, and Dana Brantley-Sieders has those in spades.” — Jenny Lawson, #1 New York Times-bestselling author of “Let’s Pretend This Never Happened”
I’m delighted, grateful, and I’m totally going to stalk visit her at The Nowhere Bookshop someday soon. Thanks, Babe!
Talking to My Tatas: A Breast Cancer Researcher’s Adventure With The Disease And What You Can Learn From It is scheduled to be published February 8, 2022!
On. My. 49th. Birthday.
I’m not one for signs, but this is the second serendipitous date associated with this book baby so far. The first was getting the offer for publication from Rowman & Littlefield on November 5 of last year, the same day I was in surgery for the first step in my left breast reconstruction. This is the second. I am filled with joy and delight!
What’s next in the process? Now that I’ve turned in finalized chapters and other components of the book with edits in response to super helpful comments and notes from editor Suzanne Staszak-Silva (shout out to my amazing literary agent Barbara Collins-Rosenberg for giving me edits and notes prior to sending them to Suzanne), the manuscript enters the production phase. I’ll be receiving notes from the Production Editor, completing any revisions, going through proofs, reaching out for endorsements – shout out to the folks who already said, “Yes, send it to me for an endorsement!” – and planning for the release and promotion.
I cannot WAIT to see the cover!
I also cannot wait until this book is available to the public, including the hundreds of thousands of newly diagnosed breast cancer patients, current patients, survivors, and caregivers. If I can help even one of those people – my survivor sisters and brothers – by informing them, inspiring them, helping them cope, or giving them a much needed laugh, then I will have accomplished something really special.
This book will also help me develop a guide for newly diagnosed breast cancer patients at my institution, another labor of love.
I send love and gratitude to all of the mentors and colleagues who’ve made me into the scientist I am today, my healthcare team for saving my life and helping me thrive, and my family for being my strength and limitless supply of love.
Wow, I haven’t posted since January??!! Shame on me! But I’ve been busy writing, and I now have a completed draft of Talking to My Tatas: A Breast Cancer Researcher’s Adventure With The Disease and What You Can Learn From It.
It feels pretty freakin’ AWESOME! I learned so much through the research, especially about the clinical aspects and how my own experience fits with breast cancer care in the United States. I also learned more about emerging therapies, disparities, and mental health related to breast cancer.
When I started this process, I had been writing fiction for about 10 years and understood more or less how to construct a story in my genre, how to query agents and small presses, how to self-publish when a particular book or story doesn’t fit with traditional publishing, and how to write blurbs (it’s HARD), synopses (it’s TORTURE), and other things that go along with the fiction universe.
When it came to nonfiction, aside from my scientific manuscripts, I had no clue where or how to start. Fortunately, I had the amazing Alice Sullivan in my corner to coach me through the process. A long time ago in a pre-COVID galaxy far, far away, I became friends with Alice, and she sent me a guide to writing nonfiction proposals. That proved to be one of the BEST tools I had in hand when I started the process for Talking Tatas.
Unlike fiction, which requires a full, complete, polished manuscript (for the most part) prior to querying agents/publishers, nonfiction requires a proposal rather than a completed manuscript. Memoirs are sometimes the exception. What is a proposal? It’s basically a plan for your nonfiction project. It includes a working blurb, detailed outline of each chapter, what makes your book stand out from other comparable titles in the market, unique selling points, a marketing plan, your credentials (or reasons for writing the book, like personal experience), and sample chapters.
A tight, well-written, carefully crafted proposal is the key to getting an agent and a publisher if you’re going the traditional publishing route. Even if you’re not, it’s a great way to map out and organize your thoughts and to be thinking about defining your target market and how you’ll reach readers in that market. If you’re planning a nonfiction project, check out these sites for proposal essentials/how to, templates, and examples of successful proposals: Nonfiction Authors Association, Reedsy Blog, Scribe Media.
Once you write the proposal and craft a killer query letter, you start the long and arduous task of sending these items to literary agents (whom you’ve selected based on research and matching interests) and hope to get some interest. It’s not speed dating, but you’re definitely looking for a connection. Be prepared for LOTS of rejections with the understanding that it’s not personal. I repeat. IT’S NOT PERSONAL. If you take rejections personally, you’re going to have a tough time in the publishing biz. That being said, if you’re lucky enough to get feedback with a rejection, put it to good use by revising your proposal. For example, I received a lot of rejections based on the fact that my proposal was cross-genre (story of my writing life/same issue with my fiction). In Tatas, I’m blending elements of memoir with the personal story and prescriptive, which is the informational component.
Ultimately, I restructured my proposal to focus more on prescriptive and less on memoir (about 80/20), and that worked!
Once you get an agent, you’ll most likely tweak your proposal again for submission to editors, perhaps having a few drafts tailored for different editors. The submission process can also be a long, arduous process, and remember, rejections are NOT PERSONAL.
Trust me – you want an agent and editor who are super enthusiastic about your work. Someone who’s lukewarm won’t be as likely to champion you, and in this very competitive business, you need champions.
While you’re querying/submitting, you should be working to build or expand your platform. This blog is part of my platform. It gives readers information to supplement what I include in the book, to showcase my style and strengths, and to hopefully connect with readers who are likely to be interested in my book. It’s also great to network with other folks who have platforms with interests that match yours. I LOVE The Bloggess and have been lucky enough to connect with her by advertising on her blog and cultivating a relationship based on fangirling and promoting her stuff. It wasn’t so much strategic as it was OMG-I-LOVE-HER-AND-EVERYONE-NEEDS-TO-KNOW-ABOUT-HER! I also adore SciBabe, A Science Enthusiast, and Sana Goldberg, so I’ve been connecting with them.
Thanks to my day job, I’ve cultivated relationships with a lot of influential people and organizations in the cancer research field and I’m forging relationships in the patient/survivor advocacy community – of which I am now a part. All of this will help me spread the word about my book, get endorsements, and hopefully make the book a success.
It’s been one hell of an adventure! Stay tuned for more. In the meantime, I’m working on a new Screw the Woo Woo post on a “spell caster” who was recommended to me on Facebook. That one’s going to be wacky and fun. Mwahahahahahaha!
First off, HUGE news! My amazing literary agent, Barbara Collins Rosenberg, landed a publishing deal for me with Rowman & Littlefield!!! I’m honored, thrilled, and still squee-ing! So, stay tuned for Talking to My Tatas: A Breast Cancer Researcher’s Adventure With The Disease And What You Can Learn From It.
Here’s the Working Blurb – it will likely change based on guidance from my amazing editor, Suzanne Staszak-Silva, but it will give you a taste of what I intend to share (my story) and spread (scientifically sound information) with this book:
Can I talk to you about my personal relationship with my breasts?
I’ve spent twenty years working as a biomedical breast cancer researcher. Then, I was diagnosed with breast cancer. I thought I knew breast cancer before it whacked me upside my left boob and left me bleeding on the curb of uncertainty. Turns out, I had a lot to learn. The purpose of this book is to share my personal adventure with breast cancer, from the laboratory bench to my own bedside, and to provide accessible information about breast cancer biology for non-scientists. I say adventure, because I’d rather think of it as an action movie with some really cool side quests instead of another tragedy-to-triumph saga. I’m not big on sagas. I am big on kickass intellectual badassery, pathological nerdiness, and talking about my sweet, sweet rack.
Why do we need another cancer memoir? In a sea of inspirational stories, celebrity survivor stories, and physician memoirs that bring a clinical perspective, nothing I’ve found in the current market tackles breast cancer through the lens of a breast cancer researcher who became a survivor. We live in an age of fake news and pseudoscience, made worse by the pervasive anti-intellectual and anti-science political culture gripping the United States and much of the world. The Internet and social media are plagued by scammers selling “alternative medicine” and woo woo “cures” for cancer. Through Talking to My Tatas: A Breast Cancer Researcher’s Adventure With Breast Cancer And What You Can Learn From It, I offer accurate, evidence-based science that is accessible to laypersons, including the more than three hundred thousand individuals diagnosed with breast cancer every year*, their caregivers, and their loved ones.
Knowledge is power, and lack of it can lead to overtreatment, unnecessary pain and suffering, and can even be deadly. By demystifying the process from mammograms, biopsies, pathology and diagnostics, surgical options, tumor genomic testing, and new treatment options, I aim to offer hope in a story intended to blend the humor and delivery style of Jenny Lawson’sLet’s Pretend This Never Happened (A Mostly True Memoir) with the integrity and scientifically sound beauty of Siddhartha Mukherjee’s The Emperor of All Maladies: A Biography of Cancer.
*American Cancer Society Facts & Figures 2020
I’ve got some work to do! In addition to writing and fleshing out chapters for my editor to review (and work her magic on), I’ve been busy working on figures and visuals for the book, cover art forms, marketing and promo plans, and getting a new headshot! The one I currently have on this page and all over the Internet is absolutely gorgeous, fun, and from 2012. A LOT has happened in 8 years, and I have aged. I’d like to think I’ve aged gracefully, but at any rate, it was time to update the image.
Lillian Boeskool is MAGIC! She made me look so good and captured the essence of my personality in a series of amazing headshots (If you’re in the greater Nashville area and need headshots or other photography, HIRE HER). I have two favorite images and I cannot decide which one to use for this page and the book. I invite y’all to enable my decision-making disorder vote for your favorite!
Photo Credit Lillian B Photography
This one on the left is super fun and catches me trying not to laugh at something funny Lillian said and/or did. It captures my mischief, my sense of humor, and really makes my face look nice.
And, unlike the previous headshot for which I straightened my hair, this one highlights my popping natural curls!
I’m almost 48 years old. Anything that makes my face look nice is gold.
Told you she was MAGIC!
Photo Credit Lillian B Photography
There’s just something about this next one on the right that speaks to me.
I think it captures my sass and tells my readers that I’m going to take them on a really funny adventure that will make them a smidge uncomfortable but will ultimately leave them laughing and glad they went along for the ride.
That’s me in a nutshell.
I can’t decide between the two!
And…just to throw a monkey wrench into this whole program…
Photo Credit Lillian B Photography
This one is my husband’s favorite.
It’s nice, too.
I’m glad he thinks I look good in all of these photographs and still thinks I’m beautiful in spite of time marching across my face and body and in spite of cancer leaving me with a janky left breast-in-progress*.
He’s pretty awesome!
I think I’ll keep him.
*Janky left breast-in-progress on display in the first two photos as the line of discoloration just above my shirt collar. Lillian asked if I wanted to Photoshop it out, but I said no. It’s where I am right now. It’s why I’m blogging, writing this book, and becoming a breast cancer patient/survivor advocate as well as a breast cancer researcher. It’s a badge of fucking honor and it stays!