It’s day 26 of National Breast Cancer Awareness month! Today, I had the opportunity to appear on the Tampa Reads segment of Fox 13 in Tampa with anchor Linda Hurtado! I was able to share my breast cancer story with a bit about science, about my personal story, and a bit about Talking to My Tatas.
It was a great experience and I hope I convinced some viewers to schedule their mammograms! Shout out to Linda Hurtado, Lisa Emerson, and the rest of Fox 13 News Team!
Cancer is a great and terrible equalizer. It doesn’t care if you’re a Democrat, Republican, Independent, or if you support other political philosophies or are apolitical. Anyone can be diagnosed with cancer. For breast cancer, access to routine screening and diagnostic imaging is critical for early detection, accurate diagnosis, and receiving treatments in a timely fashion.
It can literally mean the difference between life and death.
When breast cancer metastasizes, or spreads to other parts of the body, time is precious, and people living with metastatic breast cancer need all the financial and medical support they can get.
How can you help? There are two pieces of legislation in need of support and a federal program in desperate need of reauthorization:
The first piece of legislation, the Access to Breast Cancer Diagnosis (ABCD) Act, will reduce out-of-pocket costs for diagnostic imaging for people with health insurance. While screening mammography is normally covered, additional imaging that’s needed when something suspicious or abnormal is spotted on a mammogram can become pricey. For each of my diagnoses (initial breast cancer diagnosis and diagnosis for residual disease), I required additional diagnostic mammography, diagnostic MRI, and diagnostic ultrasound. They were most DEFINITELY medically necessary to determine that the suspicious lesions on my mammography were indeed cancer – and for past follow-up diagnostic imaging, to determine that suspicious lesions were benign. This legislation will reduce the financial burden for diagnostic imaging that can be a barrier for early diagnosis.
The second piece of legislation, the Metastatic Breast Cancer Access to Care Act, would reduce wait times for receiving Social Security Disability Benefits and Medicare. Right now, the wait time for Medicare benefits for people living with metastatic breast cancer is 5 months, and the average wait for disability is 24 months. The five-year survival rate for stage 4 metastatic breast cancer (MBC) is 22 percent, and the median survival is three years (Reference). As one legislative staffer noted when I spoke with him about the issue and the wait times, “That’s cruel.” It is. People living with MBC need medical care coverage and financial support for themselves and their families. Legislation waiving wait times for ALS and end-stage kidney disease passed, setting a precedent for this important legislation supporting MBC.
Finally, reauthorization of the National Breast and Cervical Cancer Early Detection Program, will preserve and expand access to screening for un- and under-insured American. Early detection increases a patient’s chances of survival, so this life-saving program needs your support.
Please help these Bills become Law!
Please contact your Senators and Congressional Representative and urge them to co-sponsor and/or support these three key pieces of legislation. Feel free to copy and paste information from this blog post or use it as a script in a phone call.
I’ve met and admired many survivor sisters over the years. After my diagnosis, they held me in their arms and lifted me up so I didn’t have to face breast cancer alone. Before I was diagnosed, I got to know a really cool woman named Tanisha Jones. We were represented by the same literary agency at the time, writing romance and urban fantasy* and trying to break into the fiction publishing world in a big way.
*Side note: If you’re a fan of Anne Rice and J.R. Ward, TREAT YOURSELF to Tanisha’s The Fallen Series. This exciting series is full of vampires, Fae, Weres, demons, and other supernatural beings hiding in plain sight in New Orleans. Throw in a hot homicide detective with some supernatural abilities of his own and you’ve got one helluva story!
Like me, Tanisha works in academics (one of her many jobs). She also has a daughter, just a little bit older than mine. She has hopes, dreams, highs, lows, a wicked sense of humor and a drive and work ethic to rival any I’ve seen in my almost 48 years on the planet.
Like me, she has breast cancer. Unlike me, she’s living with metastatic breast cancer (MBC). While there is no cure, she hasn’t allowed MBC to define her life or steal her dreams. She’s still writing – she published Unbound, Book 3 in The Fallen series, this month. She’s still raising her daughter. Due to health issues related to MBC, she isn’t working at the moment but she’s worked since her diagnosis in 2016.
Because America is still balking at the idea that healthcare is a human right rather than a privilege reserved only for the white and wealthy (and healthy), like many Americans, Tanisha is struggling financially due to the cost of her cancer care. I could write an entire rage post on the topics of American healthcare’s failures that include the real possibility of financial ruin, disparities in access and care, and the lack of healthcare equality and equity that is still VERY much a problem in 2020 in this country, and I will.
But right now, what matters is helping my friend who’s struggling with breast cancer.
Tanisha’s family also has a GoFundMe initiative (you know, the largest healthcare “plan” in the United States) to help her. Click here to donate what you can. It helps. It matters.
I have taken the extra book royalties I earned in November plus a small windfall that came to me at just the right time to support Tanisha. I can think of no better person in whom to invest.
Metastasis – the spread of cancer from its initial tissue of origin to another part (or parts) of the patient’s body – is deadly. Metastatic disease is, by and large, what kills people with cancer. It is an ongoing challenge for healthcare providers and researchers, and, as you may have guessed, it’s complicated.
But what exactly is metastasis? How does the process work? And why is it so hard to treat? I’ll cover what we know in this blog post, current and emerging therapies, and ongoing research designed to treat metastatic disease and allow cancer patients to survive and thrive by keeping their metastatic tumors at bay.
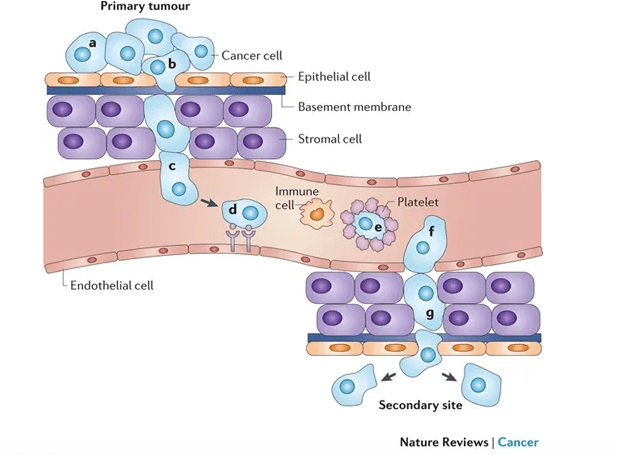
Here are the basics: tumor cells that have the ability to break away from the primary mass and invade the surrounding tissue can travel through the body via circulation (by entering the bloodstream directly or or by entering lymph nodes and from there, lymph vessels that shunt fluid back into circulation), invade a secondary organ, and begin to grow and form a new mass at the second location.
This isn’t easy for cancer cells to do. One of my grad school professors once referred to metastatic cancer cells as the decatheletes of cancer cells. Losing cell-cell contact with the tumor mass, invading the surrounding tissue, which is often a hostile environment without resources available to the primary tumor mass, is risky. Entering circulation is even more risky. The cells of origin for cancer cells are not normally equipped to withstand shear forces produced by flowing blood. They also have to avoid detection and destruction by immune cells, not only in circulation, but within the tissue of origin and within lymph nodes. Immune cells are programmed to seek out and destroy unhealthy cells, which may harbor bacterial or viral pathogens that threaten the body as a whole. Metastatic cells also have to crawl along blood vessel walls or hitch a ride on platelets, surviving in circulation without the resources available within the primary tumor mass.
From Schroeder et al. 2011 Nat Rev Can 12: 39-50.
If the metastatic cells manage to survive breaking away from the primary mass, evade vigilant immune cells, and travel through the harsh environment of the circulatory system, they face the arguably greater challenge of exiting circulation and setting up shop in an entirely different organ system that may or may not be similar to their original home. Think of them as colonists. They need to secure a space to live, gather resources from an unfamiliar landscape by competing with native cells that are better equipped because they belong, and they need to adapt and change the behavioral programs controlled by their genetic instructions in order to grow and establish a new tumor.
For breast cancer cells, common sites of metastasis include liver, lung, bone, and brain. Why those sites? One theory, the “seed and soil” hypothesis, argues that tumor cells are like plant seeds, which travel in all directions but can only live and grow if they land in compatible soil, meaning something about these particular organ environments allows tumor cells to take root. It’s an old theory, first posed by English surgeon Stephen Paget after studying autopsy records of 735 patients who died of breast cancer and spotting patterns.
During the process of invasion and metastatic spread, cancer cells experience a lot of pressures, and combined with a relatively unstable genome (covered in previous post), these pressures select for survival of cells that adapt in a process comparable to evolution by natural selection: cells that survive long enough to divide are more likely to pass favorable traits to their daughter cells. One effect of this process is that tumors formed by metastatic cells are often very different from the primary tumor, making them resistant to the therapies used to treat the primary tumor as well as other treatments. Often, they cannot be removed easily by surgery, are resistant to or quickly become resistant to chemotherapy, radiation, and targeted therapies, and grow at a rate that depletes the patient’s body of life-giving resources and causing the organs in which they are lodged to fail. In a nutshell, metastatic disease is incredibly difficult to treat.
So what can we do about it? The good news is that it is possible to manage metastatic disease in some cases, allowing patients to live longer with better quality of life. More therapies are extending the lives of patients living with metastatic breast cancer, including CDK inhibitors like Palbociclib [Ibrance; other similar drugs include Abemaciclib (Verzenio), palbociclib (Ibrance) and ribociclib (Kisqali)] that target cyclin dependent kinases that drive rapid proliferation of cancer cells, slowing their growth. Others include HER2 antibody-chemotherapy drug conjugates (delivers chemotherapy more specifically to HER2+ metastatic breast cancer cells), second-line HER2 targeted therapies, PI3-kinase inhibitors (which target a signaling pathway that is aberrantly activated in ~60% of cancers), PARP inhibitors (block DNA damage repair pathways to make cancer cells respond better to DNA damage inducing chemotherapy), and immune checkpoint inhibitors (activates T-cells in tumors and allows them to kill metastatic tumor cells) among others. See previous post for information about some of these molecular targets. For more on tumor immunology, click here.
These therapies extend the lives of metastatic breast cancer patients, but they are still a temporary fix. As mentioned above, metastatic tumor cells are tough, incredibly adaptable, and able to develop resistance to therapy. Another approach involves finding a way to induce or maintain tumor dormancy, a state in which tumor cells survive but remain quiescent rather than growing rapidly. Many metastatic lesions can persist in a state of dormancy for decades, and we do not yet understand what keeps them dormant, and perhaps more importantly, what activates their growth. But as researchers unravel the molecular mechanism that regulate dormancy and reactivation, new therapies can be developed to maintain dormancy – thus allowing cancer patients to survive and thrive during a normal lifespan in spite of their tumor burden.
Take home message: metastasis is a complex process that enables invading tumor cells to break away from the primary tumor, travel through the patient’s body, and set up shop in different organs. They are difficult to treat and are the main cause of cancer deaths, but current and emerging therapies to manage metastatic cancer are allowing patients to live longer, better quality lives.