This is the first in a series of posts dedicated to the science of breast cancer, so let’s start from the beginning with normal breast. In order to understand how cancer forms and grows, you first have to understand how non-cancerous cells behave and function. Why? Because fundamentally, cancer is an aberration of normal function. Cancer cells were once normal cells. A series of events that involve mutation in the cell’s DNA, the genetic blueprint that encodes instructions and specific modifications for that cell’s function that lead to changes in (1) the cell’s ability to divide, (2) the cell’s response to normal programmed cell death, (3) the cell’s ability to repair damaged DNA. These events reprogram the cell’s function and cause uncontrolled, abnormal cell growth, and these changes are alterations in the normal cell programs that maintain the balance between new cell growth and old cell death that maintain healthy cell function.
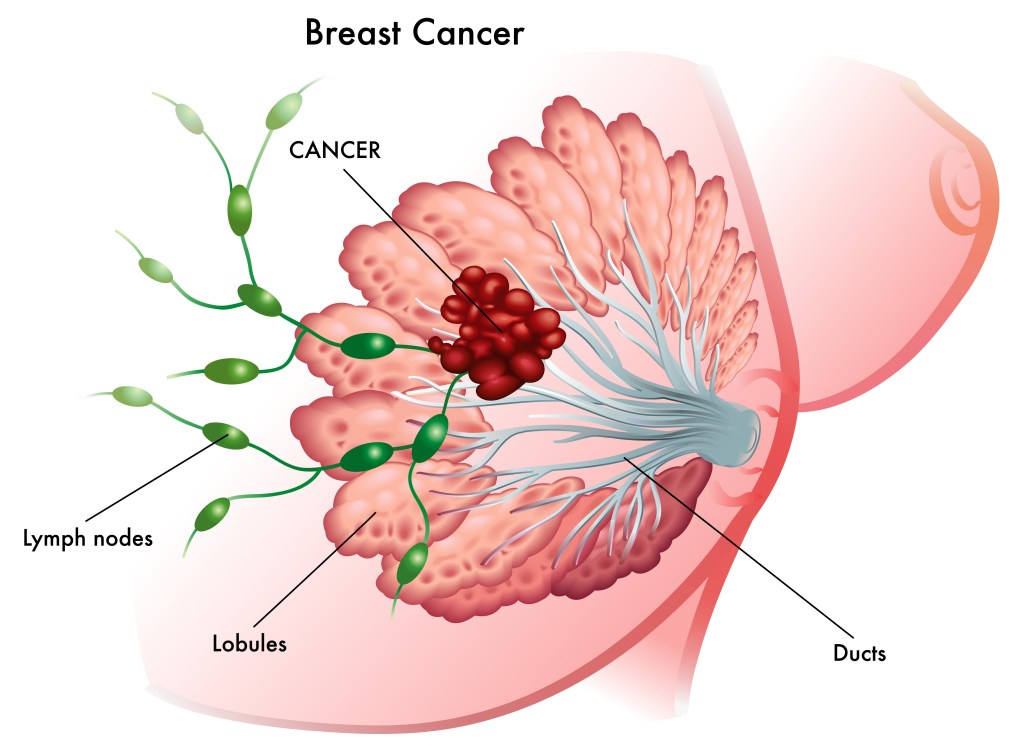
Let’s start with anatomy. Breasts are made up of milk-making (lobules) and shuttling (ducts) glandular epithelial cells anchored by connective tissue and support cells in a sea of squishy fat (adipose tissue). The glandular epithelium goes through a massive growth cycle during pregnancy and becomes a milk factory for nursing young. When the young stop nursing, the factory shuts down, most of the cells die, and the epithelium rests until the next pregnancy. The same cellular programs that control growth and death in these normal cycles become highjacked when a cell begins to transform from normal to cancer. This includes programs regulated by hormones like estrogen and progesterone, as well as cell surface growth factor receptors like HER2, which we will cover in future posts.

Most breast cancers form from ductal epithelial cells, but can form from lobular or other types of cells*. The most important take home message is that breast cancer isn’t a single disease. It is a collection of diseases classified by pathology (how it looks under the microscope) and molecular genetics (which collection of mutations in specific genes contribute to its formation and progression). There are at least five broad subtypes of breast cancer that can be further divided into additional subtypes: (1) Luminal A, which tend to be estrogen and progesterone hormone receptor positive (ER+/PR+) and lack HER2 alteration; (2) Luminal B, which tend to be estrogen receptor positive and can be HER2 positive or negative; (3) HER2-enriched, which tend to be negative for hormone receptors (ER-/PR-) and display amplification (more copies) of the gene encoding HER2 cell surface receptor; and (3) Triple negative, which lack hormone receptors (ER-/PR-) and HER2 amplification (HER2-)**. I’ll cover each of these subtypes in future posts, including the latest research on how they form at the molecular, genetic, and cell biologic level, and current/emerging treatment options.

To wrap things up, I’d like to share with you some of the work I did as a graduate student***, which involved understanding molecular regulation of normal breast epithelial development during puberty. Again, understanding how normal breast epithelium grows and forms as breasts develop is an important first step in understanding how things go wrong in breast cancer. The pictures in (A) show whole-mount preparations of mammary gland (a fancy term for squishing and flattening a small piece of tissue on a slide and staining it to show the epithelium in the sea of fat) of breast epithelium growing to fill the fat of developing breast during puberty. The specialized bulb-like structure (arrow) is called a terminal end bud (TEB). The schematic in (B) shows the structure of cells within the TEB as they grow from the TEB tip out and differentiate into their normal, mature structures in the area behind the TEB. Luminal epithelial cells line the ducts, while myoepithelial cells that surround the lumina structure contain contractile proteins that, like muscle, will eventually squeeze and contract to help milk travel to the nipple. Cap and body cells turn into these cell types when growth stops.
*American Cancer Society; **Susan G. Komen, ***From my graduate thesis

Pingback: Breast Cancer Care in the Era of Covid-19 – Talking Tatas
Pingback: Lumpectomy versus Mastectomy – I’ve had ’em both and I’m telling you all about it! – Talking Tatas
Pingback: Male Breast Cancer | Talking Tatas