It’s day 14 of National Breast Cancer Awareness Month. Whew, a blog post a day is hard, y’all! But I hope these posts have been informative, entertaining, and full of hope. We all need hope. And we all need to be inspired.
That’s what I’m aiming for tomorrow. Between the pandemic and other turmoil in the world, it’s been over 4 years since I’ve done an in-person race/walk event. I still fundraised and still kept momentum going, but there is just something about seeing a sea of supporters – people with breast cancer, survivors, caregivers, loved ones, and everyone who shows up to raise money and shine a light on this awful disease!
There’s nothing quite like it.
I’ve seen beautiful bald women and women with gorgeous scarves, women with short and long hair spray painted pink, women who’ve traded illness for the graceful bodies of athletes, women with curves for DAYS rocking it, Black, Brown, White, Asian, Indigenous, gay and all the other letters of the alphabet mafia, old, young, and men who’ve also endured this horrible disease and stand in solidarity, not to be forgotten. It’s beautiful. It’s inspiring. It gives me the will to keep going!
Please, keep going!
I walk in memory of my cousin Sherri Killian, taken from us too soon by breast cancer, my uncle Jack, who we lost to cancer, and in honor of my mother, Carol Brantley, survivor. I walk in honor of my bestie Pam Jasper, and my friends Sue Daugherty Draughn, Linda Horton, Janet Piper, Karen Pugh, Tanisha Jones, and so many others who are more private about their cancer stories. So many family members, friends, colleagues, and acquaintances have been touched by cancer. We all know someone.
Sometimes we are that someone.
I walk for you. I may not know you personally, but we are connected. I work for you. I will not rest. If I can help one person, it is worth it. We fight cancer by holding one another up, celebrating victories, and witnessing and remembering those who leave us too soon. We fight.
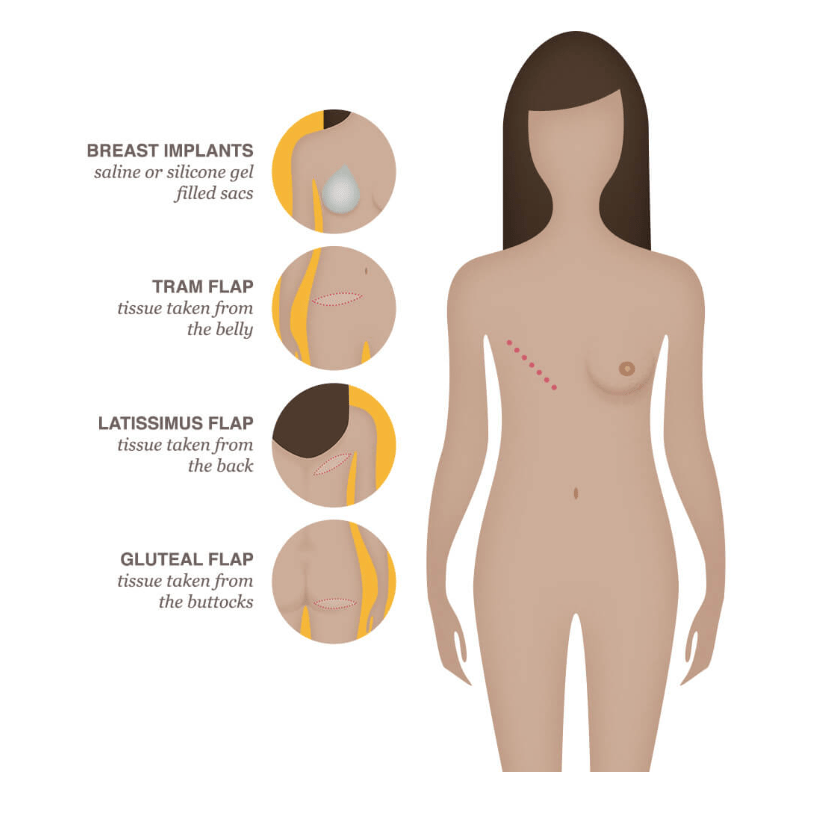
It’s day 13 of National Breast Cancer Awareness Month! Today, I’m taking a break from the usual programming to talk about my breast reconstruction journey, which I hope is (finally) over. I had the misconception that breast reconstruction was relatively simple, one or two procedures and done!
Image Source Here. Also has information about different types of reconstruction!
Yeah, that was before I got breast cancer. Oncoplastic reconstruction (lumpectomy followed by reduction and lift) was a one and done, as is (or can be) aesthetic flat closure (going flat). But building new breast(s) after mastectomy is complex and involves multiple surgeries/procedures to achieve symmetry and an aesthetically pleasing result. That’s where I’m at in the process.
I talk about this in Talking to My Tatas, and include pictures of where I was in the process as of 2021, but it might be useful to include a timeline and description of the various procedures I’ve had. Everyone’s reconstruction process is unique and tailored, but it should give you an idea of how involved the process can be and often is for people who’ve been diagnosed with breast cancer.
June 2018 – Tumor removal from left breast by lumpectomy and oncoplastic reconstruction
September 2018 – Radiation therapy on left breast
February 2020 – Diagnosed with residual disease in the left breast (at the beginning of the Covid-19 pandemic)
May 2020 – Unilateral mastectomy to remove left breast and to implant expander
(Involved several intervening procedures like 3X saline fills for expander and physical therapy to regain mobility after mastectomy, which was compounded by radiation damage to the skin over my left breast and breast tissue)
November 2020 – DUG flap reconstruction (grafting of thigh and muscle/skin tissue from right thigh to build foundation of left breast plus mastopexy (reduction and lift) on right breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
February 2021 – Liposuction and fat grafting into left breast + more tweaking on the right breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
July 2021 – Liposuction and fat grafting into left breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
December 2021 – Liposuction and fat grafting into left breast and scar revision on right breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
October 2022 – Liposuction and fat grafting into left breast and minor scar revision on right breast
Image Source Here. Also has information on thigh flap reconstruction procedures.
That’s seven procedures, not counting biopsies and a lumpectomy from 2016 to remove a benign papilloma, in two years since residual disease detection. It’s a LOT! I count myself lucky to have a brilliant surgeon who has worked with me at my pace to get symmetry between a mostly natural right breast and reconstructed left breast, which is no easy task. And I have a great support system. But it’s a LOT. Each surgery involves recovery from anesthesia, incisions, bruises a plenty (lipo is brutal) and the mental and emotional impacts (which included depression and hypervigilance that made me feral). That required therapy, another part of the process.
Is it worth it? For me, the answer is yes. I’m almost back together and beyond amazed and pleased with how I look and feel. I am whole. Not the same, never the same, but whole. It’s a process. Remember that when you’re checking in with your survivor friends who may be waiting for follow-up procedures, tattoos or surgical nipple-building procedures, trimming of excess skin around incision areas, etc. It’s a process. Be kind. If you’re a survivor in the thick of reconstruction, remember to be kind to yourself and that YOU ARE WORTH IT!
While most breast cancers are sporadic, meaning there’s no genetic predisposition (i.e. gene variant inherited from one or both of your parents that increases your risk of breast cancer) that caused the cancer, around 5-10% of breast cancers are thought to be familial. Knowledge is power, and knowing if you have a genetic risk for breast cancer can empower you to take charge of your health by surveillance and managing your risk.
How do inherited gene variants increase a person’s risk for breast cancer? Everyone has two copies of genes that we inherit from our parents. These genes have many different variants in the human population, and some specific gene variants are associated with increased risk of breast cancer. For example, inherited mutations in BRCA genes that make the gene product non-functional (i.e. no longer able to repair damage to DNA) increase the risk for breast and other cancers because the loss-of-function allows other mutations to build up in affected cells, which can eventually transform them into cancer cells. If you carry BRCA variants associated with cancer, you may be at greater risk and you can also pass these risk genes to your children.
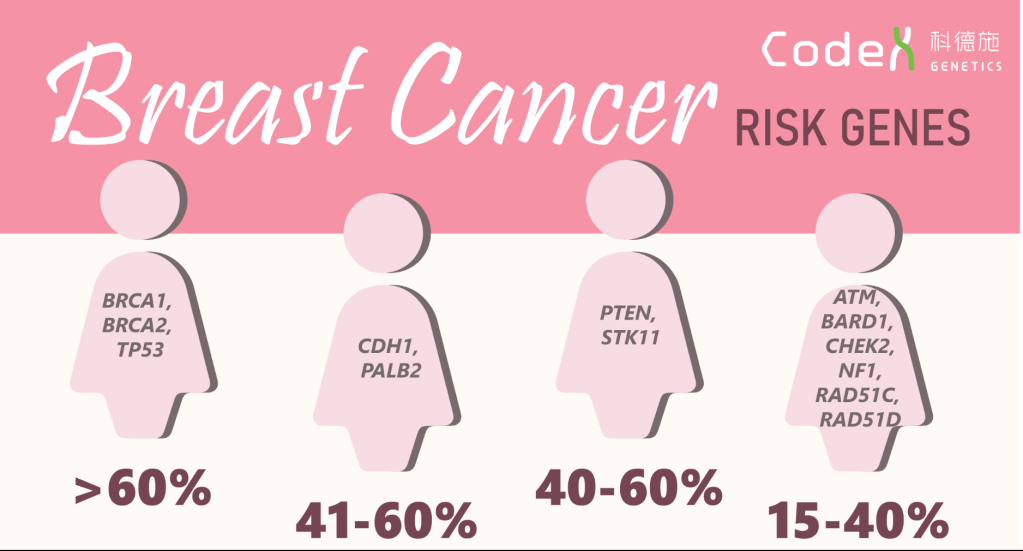
In addition to BRCA1 and 2 genes, other inherited gene variants have been identified that are associated with increased risk for breast cancer, as shown in the graphic below. Some of these genes, like TP53, PTEN, STK11, CHEK2, NF1, produce proteins that are also involved in regulating cell growth, so non-functional variants cannot put the breaks on cell growth and can cause cancer cells to grow uncontrollably. The PALB2, BARD1,ATM, and RAD51D gene products work like BRCA gene products to repair DNA damage, so loss of function increases the chance of accumulating mutations in cells, which can lead to cancer. The RAD51C gene product is involved in stopping cells with DNA damage from growing, so loss of function allows cells with mutations to divide and accumulate more mutations, which can lead to cancer.
Image Source Here. Percentages represent relative risk of breast cancer for people who have these gene variants associated with breast cancer.
Should you get genetic counseling and genetic testing? That’s a personal decision, but here are some recommendations from the CDC that might help you make your decision:
A strong family history of breast and ovarian cancer,
A moderate family health history of breast and ovarian cancer and are of Ashkenazi Jewish or Eastern European ancestry.
A personal history of breast cancer and meet certain criteria (related to age of diagnosis, type of cancer, presence of certain other cancers or cancer in both breasts, ancestry, and family health history).
A personal history of ovarian, fallopian tube, or primary peritoneal cancer.
A known BRCA1, BRCA2, or other inherited mutation in your family.
Knowing your risk can help you and your healthcare providers make decisions about surveillance and possible interventions. Take care of yourself, and if you can, find out about your family history of breast cancer.
It’s day 11 of National Breast Cancer Awareness Month! I’ve been so inspired, entertained (laughter is often the best medicine), and filled with pride by social media activity showcasing people working hard to raise breast cancer awareness, celebrating survivors, and sharing their stories!
Here are a few of my favorite videos for National Breast Cancer Awareness Month!
Indigenous Peoples Reminding Their Loved Ones to Book Their Mammograms!
This video featuring funny stories from deaf breast cancer survivors lit me up!
Funny stories from 4 deaf breast cancer survivors!
On of my favorite comedians, the incomparable Tig Notaro, tells us how to make breast cancer funny!
Tig is the BEST!
And last but not least, here’s a great story from another favorite comedian, the amazing Wanda Sykes!
It’s nice to not need a bra!
Got any favorites? Send me links! Sharing is caring, and we could all use a laugh!
It’s day 10 of National Breast Cancer Awareness Month! Today is all about raising funds to support the vital mission of non-profits devoted to eradicating breast cancer! This year, I’m raising funds for Susan G. Komen through the Greater Nashville More Than Pink Walk!
Help me reach my goal!
***Note: I am a Komen employee, but my fundraising is part of my personal advocacy work outside of the organization, and opinions expressed in this blog are my own. I do not speak for Komen here.***
You can support my fundraiser HERE! My goal is to raise $1,000!
Why fundraising? Because I understand how important the mission is for patients, survivors, caregivers, and loved ones who have been affected by breast cancer. As a breast cancer researcher, funding was the number one priority for me in my lab. Without funding to pay for qualified personnel, supplies, infrastructure, and other items necessary to keep a state-of-the-art laboratory running, innovations and treatments of the future can’t happen.
As an advocate and survivor, I understand how important advances in screening, diagnostics, treatments, and survivorship are for survivors like me and for future survivors. I benefitted from advanced surgical and molecular diagnostic technologies, and I know that if my cancer comes back, there are so many more treatment options to keep me alive and thriving.
Being in the field, I understand that inequities and inequalities in breast cancer screening and care plague our nation in communities of color, in LGBTQIA+ communities, in people with disabilities, and in poor and un/underinsured communities. Fundraising for organizations that make eliminating disparities a vital part of their mission is key to make sure everybody has an equal and just opportunity to be as healthy as possible.
Fundraising also helps me feel empowered. Everyone’s breast cancer experience is unique. For me, the feeling of helplessness was one of my biggest challenges. Working to eradicate breast cancer through advocacy and fundraising has helped me take back my power. And it gives me hope! We could all use that!
Please support your favorite breast cancer charity for National Breast Cancer Awareness Month! Every donation matters!
And stay tuned for pictures from the More Than Pink Walk. I’ll be rocking pink hair and a pink boa to celebrate!
It’s day 9 of National Breast Cancer Awareness Month! Today, let’s cover breast cancer and how it affects the LGBTQIA+ Community—Lesbian Gay Bisexual Trans Queer/Questioning Intersex Asexual Plus other gender identities outside of Cis Heterosexual (Straight). Cancer doesn’t discriminate, but people, particularly those in power, can and do. Fortunately, there are resources available to help people in these communities navigate the healthcare system, including cancer care. My focus is on breast cancer, but some of the resources provided in the list below are more general and include multiple types of cancer care.
LGBTQIA+ people often experience discomfort and discrimination during healthcare encounters (and in the current political climate, in their communities and at the hands of politicians who challenge their very right to exist), which may account for reduced odds of receiving annual mammography screenings among some members of the community. This is especially true for trans persons who experience difficulty finding providers who understand their unique needs and who can or will perform appropriate screenings (e.g. breast and pelvic exams for trans men, prostate exams for trans women). One glaring example from my neck of the woods is a recent attack on Vanderbilt University Medical Center’s Transgender Clinic by Republican state legislators. Early detection is key to a positive outcome when it comes to cancer, and anything that creates a barrier to seeking and receiving essential health screenings, including bigotry, can cause unnecessary pain, suffering, and death.
LGBTQ populations have the highest reported rates of tobacco and alcohol use compared to non-LGBTQ populations, which increases cancer risk and correlates with a disproportionate number of LGBTQ individuals living with cancers, including anal, breast, cervical, colorectal, endometrial, lung, and prostate (click here for reference). The intersection of identities (race/ethnicity, disability, cultural) and socioeconomic status compounds inequities in care and screening and disparities in survival and quality of care and life (click here for reference). Clearly, there is need for accessible and tailored cancer care for LGBTQIA+ populations in every location. The same issues with insurance coverage, transportation and accessibility, and availability of care that plague urban and rural communities, respectively, still apply.
What’s available now? There are several resources to help LGBTQIA+ persons with cancer screenings and cancer care. Not enough, but the ones in place are a great start:
It’s day 8 of National Breast Cancer Awareness Month! Breast cancer is widely considered to be a disease of biological females (e.g. cis women, intersex people), though cis men, trans men who forgo top surgery and trans women can develop breast cancer, as can non-binary, gender fluid, and literally any human being. That’s because we all are born with a small amount of breast epithelial tissue—cells in the breast that can grow, develop, and eventually produce and deliver milk to nursing infants.
Weird quirk of biology, but that’s how it goes. We all have a little breast tissue (unless we get it removed), so we can all theoretically get breast cancer. In the figures below, you can see a schematic of how epithelial tissue appears at birth and how it grows in response to hormone signals during puberty, as well as how the network of epithelial tissue from a mouse actually looks under a microscope. For more on how the process works, see my previous post on breast anatomy, structure, and function.
**Note – mice and other mammals have mammary epithelial tissue to make milk, which is one of the defining characteristics of a mammal, and the growth and development of mouse mammary epithelium is very similar to that in humans.**
During puberty, biological female breast epithelial tissue grows in response to female hormones like estrogen and progesterone. For biological males, the epithelium doesn’t grow in response to male hormones like testosterone, leaving only a small cluster of epithelium behind. Since biological females grow more epithelium and are exposed to hormones that make these cells grow, they have a greater risk for developing breast cancer. But biological males are still at risk, since the small amount of breast epithelium left behind after puberty can become cancerous.
How does this happen? First of all, the number one risk factor for cancer in general is age. See my previous blog posts, Intro to Cancer and Cancer 101, for how normal cells become cancer. CNN version – it involves random mutations in DNA that alter genes that tell cells to grow and/or in a small percentage of cases inherited gene variants like BRCA1 and BRCA2 (see previous post on how BRCA genes work). If enough of these mutations accumulate over time in a breast epithelial cell, that cell can transform into cancer.
While more rare in biological males, get enough mutations in a breast epithelial cells and you get male breast cancer. About 1 in every 100 breast cancer cases diagnosed in the United States is found in a man. According to the CDC, risk factors include: getting older, genetic mutations and a family history of breast cancer, previous radiation therapy in the chest area, hormone therapy treatment for prostate cancer, Klinefelter syndrome (in which a person has an extra X chromosome), some conditions that affect the testicles (like injury or removal), liver disease, being overweight, and being obese.
If you have a family history of breast cancer and ovarian cancer, consider genetic counseling and testing for BRCA1 and BRCA2 variants associated with increased risk of breast cancer. In men, mutations in these genes can increase the risk for breast cancer, prostate cancer, and pancreatic cancer (see CDC).
As with female breast cancer, early detection and diagnosis is key for a good prognosis. Pay attention to your body and any changes in your breast area, and look for symptoms including:
A lump or swelling in the breast. Redness or flaky skin in the breast. Irritation or dimpling of breast skin. Nipple discharge. Pulling in of the nipple or pain in the nipple area.
Also, don’t let stigma, shame, or toxic masculinity keep you from seeking help and advice from your healthcare provider. Since male breast cancer is rare, you may feel like you’re alone, but there are resources and survivor networks available to help, ones that are decidedly not pink and are tailored for men. Ask your healthcare provider about local and online support groups, mental health support, and other resources. For more information on male breast cancer, check out these resources: Breastcancer.org, The National Cancer Institute, The American Cancer Society, The National Breast Cancer Foundation, Susan G. Komen.
It’s Day 7 of National Breast Cancer Awareness Month! Being on the receiving end of a breast cancer diagnosis is terrifying. Believe me, I’ve been there, done that, and have the internal and external scars to prove it. Navigating the healthcare system to find someone with answers who can tell you what type of breast cancer you have and how best to treat it can be a challenge. And standard of care treatments like chemotherapy and radiation cause major anxiety due to their side effects. It is tempting to look for treatments that will work without side effects.
Scammers prey upon anxiety, fear, and desperation to peddle “alternative treatments” that have not been clinically tested and for which there is no evidence to support anti-cancer properties. These so-called treatments do nothing to stop the cancer from growing and do not kill cancer cells in the body. Some may actually cause harm. And the costs are astronomical.
Quick note: This post is about “Alternative Medicine,” not “Complementary Alternative Medicine.” They may sound alike, but they are two very different things. “Complementary Alternative Therapies” are used in addition to standard of care cancer treatments and are monitored by healthcare professionals. These may include mindfulness meditation, yoga, and acupuncture among others. Spiritual practices may also be complementary alternative therapy approaches. These are fine to try so long as you let your healthcare provider know about them and as long as you take your standard of care medicines or treatments.
By contrast, “Alternative Medicine” scam artists actively discourage conventional standard of care treatments in favor of their woo woo treatments. I’ve covered a variety of woo woo scams on this blog, but when I found this one, I was livid. There are actual “clinics” in Mexico that offer alternative therapies, charge exorbitant prices for them, and cause harm and quite possibly death to desperate cancer patients.
***Note: this is not a dig at legitimate hospitals and cancer treatment centers located in Mexico***
I refuse to link these so-called practices, but they go by names like “Oasis of Hope,” specializing in “Holistic and Alternative Cancer Treatment” like oxygenation therapy (doesn’t do a thing for cancer), hyperthermia (can help other cancer treatments like radiation and chemo work better but isn’t meant to be used alone), vitamins and supplements (see previous post), ozone autohemotherapy (which is not approved by the FDA and is classified as a toxic gas with no known useful medical application in specific, adjunctive, or preventive therapy) and “natural cancer treatments” that they do not define but their white papers (not peer reviewed or published in scientific journals) mention intravenous curcumin (covered in a previous post) and vitamin K (see previous post on antioxidant and supplement therapies). Spoiler alert: these “therapies” have not been shown to be effective at treating breast cancer in clinical trials. Worse, these are on a subpage marketed to people with stage IV breast cancer, some of the most vulnerable people living with cancer. And they do not accept insurance, being located in Tijuana, Mexico, so patients must pay out-of-pocket. For Oasis of Hope, costs range from $19,000 for 18 days of treatment to $29,950 for an “enhanced” experience that lasts 20 days.
Another dubious clinic in Tijuana called “Immunity Therapy Center” is run by a man named Dr. Bautista. He, too, offers alternative treatments much like those from Oasis of Hope in addition to bovine and shark cartilage (not FDA approved for cancer treatment), magna rays (whatever that’s supposed to mean), and “detox,” something your liver does for you normally so you really don’t need specialized chelators and vitamin supplements to do it. As for the immune therapy, the dendritic cell vaccines described on the website are being testing in clinical trials for breast cancer in the United States, but they are not currently approved and we don’t yet know if they really work. That’s another insidious way scammer deceive cancer patients – they use jargon and buzz words from legitimate medical treatments to lend themselves false credibility.
These types of “clinics” are everywhere, not just Mexico. Using a simple Google search, I found them in Arizona, Minnesota, California, Tennessee, the United Kingdom, Georgia, and Illinois on the first page. Many were marked as ads, which is another red flag.
So how do you know if you’re receiving information about legitimate cancer treatments versus scams? This handy video guide from the National Cancer Institute is a great place to start. First and foremost, talk to your doctors and healthcare providers, who should be licensed, board certified, and have expertise in breast cancer diagnosis and treatment. And remember, if something sounds too good to be true, it probably is.
It’s day 6 of National Breast Cancer Awareness Month. I’m creating a new post every day in the Month of October to spread awareness, information, accessible science, practical advice, and humor. I can write about the science of breast cancer all day, and I’ve got plenty of stories to tell and woo woo bullshit to debunk, but I really want to hear from y’all.
What do you want to know about breast cancer, breast health, breast biology, treatments, surgeries, radiation, or any topic? Want me to investigate something a friend told you would help with your cancer, or some off the wall thing you found on FaceBook? Need resources on getting screening mammograms, including financial assistance, and on getting breast healthcare? Want to see pictures of my cats and hear about how they’ve kept me entertained and happy during my breast cancer years?
Let me know!
I’m a research whore – send me down a rabbit hole and help me find something new! Comment on this post with what you want to know and I’ll select three folks at random to receive a signed copy of Talking to My Tatas, my breast cancer book.
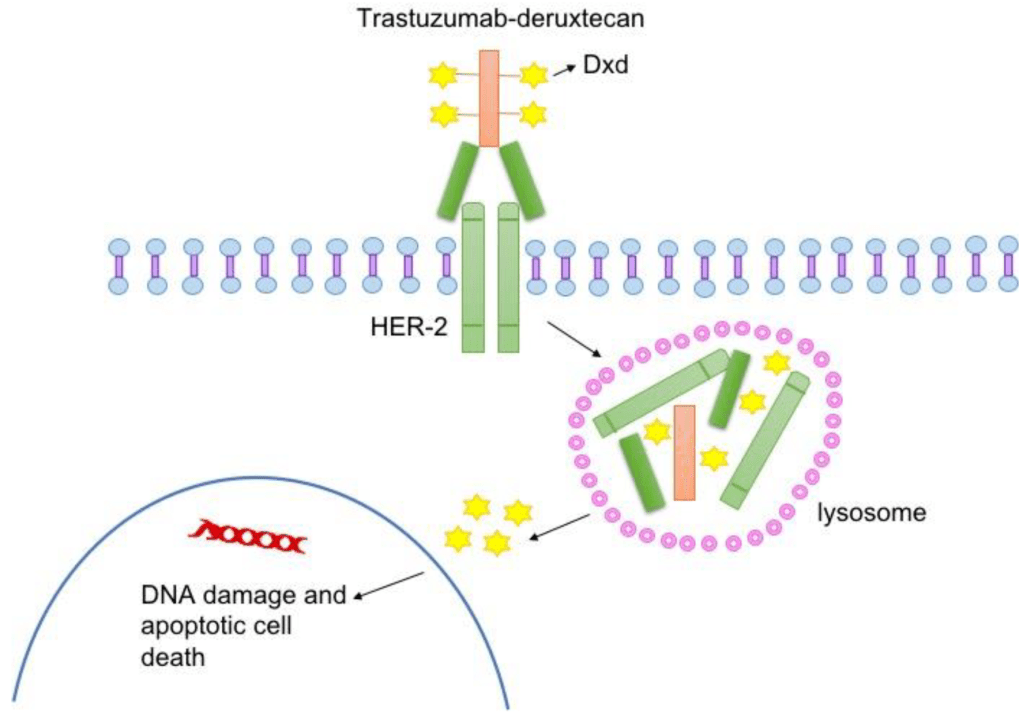
For today’s topic, let’s talk about the DESTINY-4 clinical trial that represents a HUGE advance in breast cancer treatment options for people with HER2-low advanced cancer. As I discussed in my previous post about breast cancer subtypes, HER2+ breast cancers are diagnosed based on how they look under the microscope and if they have extra copies of the gene that makes the HER2 cell surface receptor protein and/or if they express higher than normal levels of HER2, a protein that makes breast cancer cells grow uncontrollably.
The standard of care is to classify HER2+ breast cancers as meeting a threshold for HER2 receptor expression. Cancers that express levels of HER2 below that threshold were considered HER2-negative and not treated with HER2 targeted therapies. But people with low levels of HER2 in their breast tumor could still benefit from HER2-targeted therapies. To test that hypothesis, Dr. Shanu Modi, MD, of the Memorial Sloan Kettering Cancer Center led a clinical trial that tested an antibody drug conjugate called Trastuzumab Deruxtecan (T-DXd) to see if patients with HER2-low metastatic breast cancer benefitted from this treatment. This drug consists of trastuzumab, an antibody that binds to HER2 on tumor cells, and a toxic drug that is delivered directly to the tumor by trastuzumab, which kills cancer cells. People who received this drug in the trial lived longer and had a longer time before their cancer progressed compared to patients who received chemotherapy. The drug reduced tumor burden, the amount of cancer in the body. The major side effects of treatment with this drug include heart and lung function issues, which need to be closely monitored in people taking this drug.
Not only do these results provide hope and more treatment options for patients with metastatic breast cancer, they will likely change the way we classify breast cancers by molecular subtype, adding HER2-low to the classification system. Ongoing clinical trials will test this drug on patients with different levels of HER2 expression to determine the range of expression that defines HER2-low tumors likely to respond.
To learn more about Trastuzumab Deruxtecan, visit the National Cancer Institute website. Click here for more information about breast cancer treatment clinical trials.
It’s the fifth day of National Breast Cancer Awareness Month 2022! Quick update from yesterday – my (hopefully) last breast reconstruction procedure went great! I’m home recuperating and enjoying love from my fur babies and my family. I haven’t looked at the result yet, but the left side of my surgical bra looks fuller. Hooray!
Now, back to the subject of breast cancer molecular subtypes! To recap, breast cancer isn’t a single disease. It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
Molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment, include four subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer TNBC.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about the triple negative subtype, which do not express hormone receptors for estrogen and progesterone and also do not express express a cell surface protein receptor called HER2. That’s how it got its name, triple negative, because of the three receptors it does not express. These breast cancers have other ways of growing abnormally that don’t involve hormones or HER2, and they tend to grow very fast. For example, some TNBCs have higher higher than normal levels of EGFR receptors, which are in the same cell surface receptor family as HER2. Like HER2, EGFR normally tell breast cells to grow during normal development in puberty. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Aside from targeting EGFR, a strategy being tested in clinical trials, people with TNBC have fewer treatment options with targeted therapies (therapies that inhibit hormone receptors and HER2) than other subtypes.
Aside from EGFR receptors, what make TNBC cells grow? There are several molecular pathways that become altered in TNBC. These pathways often function in normal breast epithelial cells telling them to grow when appropriate (cell surface receptors like EGFR, FGFR, and CSF1-R). When receptors on the surface of the cell becomes activated, they send signals to the breast cell that tells it to grow, like when your breasts are growing during puberty. Normally, after puberty, the receptor and related receptors are no longer activated and your breast cells stop growing. In breast cancer, your breast cells make too many receptors, which become constantly activated, making your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these receptors make the cancer cells grow uncontrollably.
One interesting characteristic of TNBC is that this subtype often has more interactions with the body’s immune system, meaning that immune cells travel to the tumor, get inside of it, and try to kill cancer cells and eliminate them from the body. Many cancer cells develop defenses against the immune system, using cell surface proteins like PD-1, PD-L1, and CTLA4 to shut down the immune cells. Tumors with lots of immune cells, called immunologically “hot,” may respond well to immune therapies that block the activity of PD-1, PD-L1, and CTLA4. The drug Pembrolizumab, which targets PD-1, is used to treat advanced TNBC. The drug Sacitiuzumab Govitecin was recently approved to treat TNBC. More on that below!
TNBC breast cancer is not as common as HR+ breast cancer, accounting for 15-20% of breast cancers. However, these breast cancers are often more aggressive and faster growing than HR+ breast cancer. They also disproportionately affect younger women and women of African descent. They are diagnosed by a pathologist based on analysis of gene and protein expression if ER, PR, and HER2 present in cancer cells in a biopsy and in the tumor after surgical removal. Low or no expression of these three receptors leads to a diagnosis of TNBC. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor.
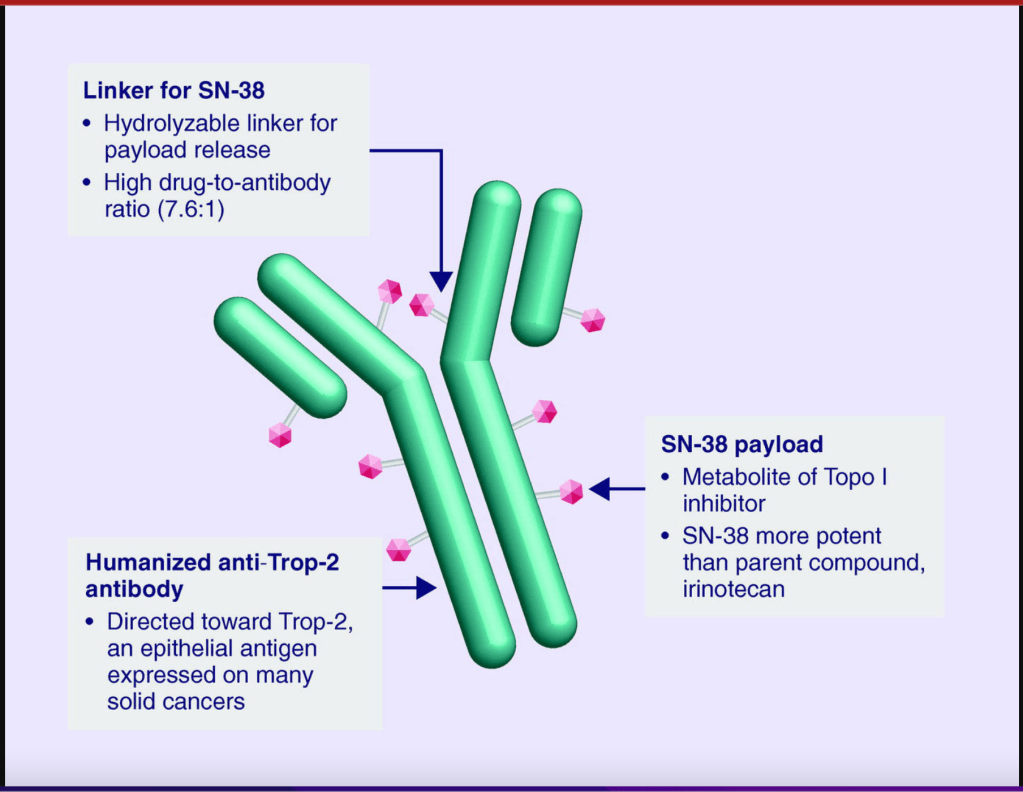
Follow-up treatments include chemotherapy, which was the only option for people diagnosed with TNBC for many decades. Recently, drugs developed specifically to treat TNBC have been approved and are being used in the clinic and undergoing additional testing in clinical trials to refine and optimize their ability to work with other drugs to kill more cancer cells. I discussed Pembrolizumab above. Let’s go over a little bit about Sacituzumab Govitecan. This drug binds to the cell surface protein Trop-2. Many TNBCs have higher than normal levels of Trop-2 on the surface of their cells. Sacituzumab Govitecan, approved in April of 2022, as a treatment for metastatic TNBC, is an antibody-drug conjugate that uses the an antibody against Trop-2 to carry a toxic drug directly to breast cancer cells with high levels ofTrop-2, targeting tumor cells and reducing damage to normal cells and tissues.
These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on TNBC, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams. Though TNBC is trickier to detect, screening mammography remains a vital tool for early detection of TNBC and other breast cancer cell types.