I can’t believe I have to write this post. I’m shaking my head and weeping for the future of humanity as I write it. Are people really stupid enough to believe that ivermectin – a drug we use in our laboratory mice to treat pinworms (butt worms) – can cure Covid?
Yes (sadly). Yes, they are.

Ivermectin is used to treat butt worms in animals. It can also be used to treat roundworms in people. It works by paralyzing worms, specifically by binding to proteins on motor neurons (nerves that tell muscles to move) and disrupting their activity. It also mucks around with the ability of nematode worms to reproduce.

Fun fact: the naturally occurring analogs of ivermectin, avermectins, were discovered in bacteria from soil samples collected by Dr. Satoshi Ōmura from woods near a golf course in Kawana, on the south east coast of Honshu, Japan. The name “avermectin” reflects the activity of these compounds, making treated organisms “worm free.” Dr. Ōmura and Dr. William Campbell shared the 2015 Nobel Prize in Physiology or Medicine for this discovery. You can read more about that here. Ivermectin in pill form can be used in humans to treat parasitic worms, and topical (on the skin) formulations are also used to treat head lice and rosacea.
It does actually have other, non-butt worm related activities that include treatment of severe muscle spasticity in patients with spinal cord injuries and shows activity against leukemia in laboratory animal models. It may also target molecular pathways relevant to treatment of other cancers, including lung and colon cancer and glioma based on laboratory animal studies, and could block inflammatory T-cell activity in atopic dermatitis, relieving irritation. A recent review covers the research on these applications.
Okay, given these other potential applications, I guess I can kinda sorta see why some folks without a science background might be buying into the idea of using Ivermectin to treat Covid, but(t) still…
This apparently became trendy because of ongoing clinical trials designed to test the efficacy of Ivermectin for Covid-19 treatment and prevention, alone and in combination with other drugs.
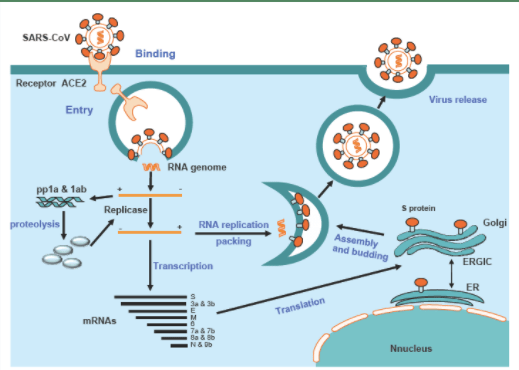
Why? Because laboratory studies (in petri dishes in a lab, NOT in people) have shown that Ivermectin can inhibit viral replication, which means it can stop the virus from making copies of itself, which is how it spreads. In vitro. In vitro means “performed or taking place in a test tube, culture dish, or elsewhere outside a living organism.” Plenty of other previous studies showed that ivermectin blocks replication or interferes with the production and spread of other viruses, including HIV, Dengue virus, West Nile virus, and a few others. In vitro. You can review some of these studies here. In spite of these in vitro studies, there is no evidence that ivermectin has any anti-viral effect on the SARS-CoV-2 virus that causes Covid-19. For a link to clinical trial data, click here.
And misuse of ivermectin can be dangerous. According to the FDA, “Even the levels of ivermectin for approved human uses can interact with other medications, like blood-thinners. You can also overdose on ivermectin, which can cause nausea, vomiting, diarrhea, hypotension (low blood pressure), allergic reactions (itching and hives), dizziness, ataxia (problems with balance), seizures, coma and even death.”
The best way to limit the spread of SARS-CoV-2 is to get the vaccine. Period.
And Now for the PSA I never thought I’d have to make…
About the whole so-called “urine therapy” thing – something I never in a million years imagined I would blog about. It isn’t a thing. Apparently, some anti-vaxx conspiracy theory wingnut named Christopher Key has been encouraging his followers to drink their own urine to ward off the SARS-CoV-2 virus instead of getting vaccinated.
What. The. Fuck.!?!?
Spoiler Alert – urine does fuck all for COVID-19.

For the sake of being thorough and due diligence, I performed a PubMed search for “urine therapy covid” on January 16. The search produced 188 results, most dealing with the effects COVID-19 on kidney function, studies related to the potential spread of the virus through urine (risk reported to be negligible), urine-based COVID-19 testing and analysis of cytokines and other diagnostic markers, and testing for SARS-CoV-2 in waste water.
The funniest result was a paper with the title, “Influence of perceived threat of Covid-19 and HEXACO personality traits on toilet paper stockpiling” published in PLoS One.
This one was more sad than funny, but apparently some folks in India are using cow dung to treat COVID-19. People…rubbing animal shit and urine all over your body isn’t effective at treating ANYTHING and is likely to expose you to a whole lot of nasty zoonotic (spread by animals) diseases. Plus you’ll stink. Just…don’t.
You know what I didn’t find in my literature search? I didn’t find a single peer-reviewed study endorsing the use of drinking your own piss as a treatment for COVID-19. Zero, zip, zilch, nada – no evidence to back up this ridiculous claim.
Not that the crazies need silly things like evidence. This actually fits quite nicely with the all-natural woo woo trends. Can you picture it? All natural, locally sourced, sustainably harvested on tap pee pee for your health needs! You’ve heard of eating placenta (don’t do that, either), but why stop there? Drink your pee! When it’s fresh, it looks like a beer.
Sure doesn’t taste like beer. Stick to drinking nice, cold brewskies, and get your vaccine. Please.