It’s day 6 of National Breast Cancer Awareness Month. I’m creating a new post every day in the Month of October to spread awareness, information, accessible science, practical advice, and humor. I can write about the science of breast cancer all day, and I’ve got plenty of stories to tell and woo woo bullshit to debunk, but I really want to hear from y’all.
What do you want to know about breast cancer, breast health, breast biology, treatments, surgeries, radiation, or any topic? Want me to investigate something a friend told you would help with your cancer, or some off the wall thing you found on FaceBook? Need resources on getting screening mammograms, including financial assistance, and on getting breast healthcare? Want to see pictures of my cats and hear about how they’ve kept me entertained and happy during my breast cancer years?
Let me know!
I’m a research whore – send me down a rabbit hole and help me find something new! Comment on this post with what you want to know and I’ll select three folks at random to receive a signed copy of Talking to My Tatas, my breast cancer book.
For today’s topic, let’s talk about the DESTINY-4 clinical trial that represents a HUGE advance in breast cancer treatment options for people with HER2-low advanced cancer. As I discussed in my previous post about breast cancer subtypes, HER2+ breast cancers are diagnosed based on how they look under the microscope and if they have extra copies of the gene that makes the HER2 cell surface receptor protein and/or if they express higher than normal levels of HER2, a protein that makes breast cancer cells grow uncontrollably.
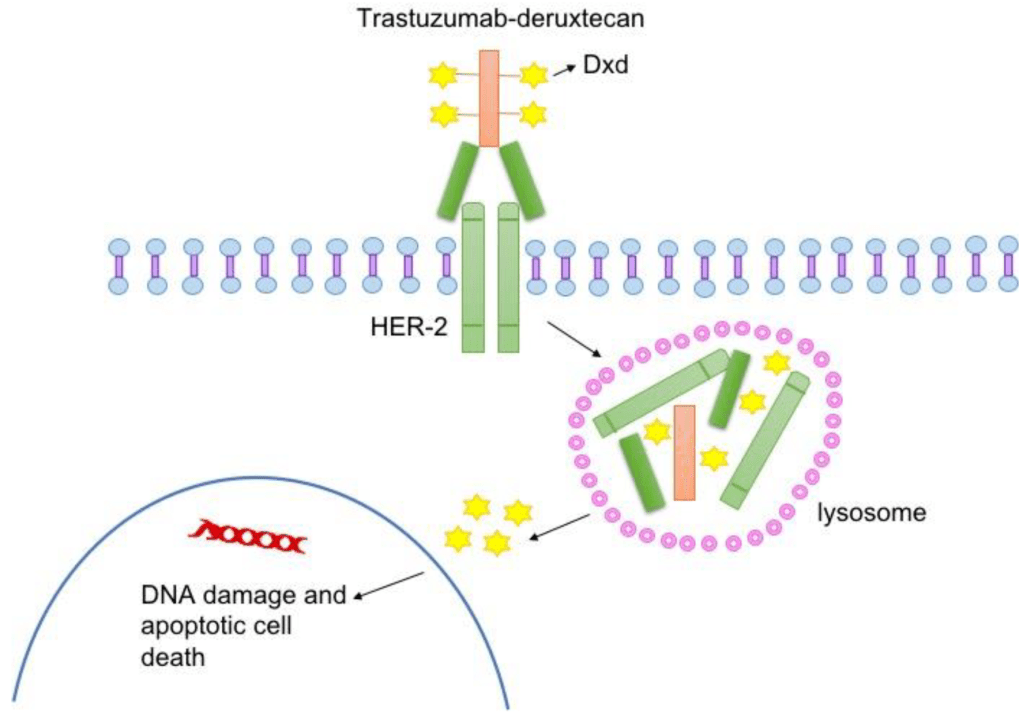
The standard of care is to classify HER2+ breast cancers as meeting a threshold for HER2 receptor expression. Cancers that express levels of HER2 below that threshold were considered HER2-negative and not treated with HER2 targeted therapies. But people with low levels of HER2 in their breast tumor could still benefit from HER2-targeted therapies. To test that hypothesis, Dr. Shanu Modi, MD, of the Memorial Sloan Kettering Cancer Center led a clinical trial that tested an antibody drug conjugate called Trastuzumab Deruxtecan (T-DXd) to see if patients with HER2-low metastatic breast cancer benefitted from this treatment. This drug consists of trastuzumab, an antibody that binds to HER2 on tumor cells, and a toxic drug that is delivered directly to the tumor by trastuzumab, which kills cancer cells. People who received this drug in the trial lived longer and had a longer time before their cancer progressed compared to patients who received chemotherapy. The drug reduced tumor burden, the amount of cancer in the body. The major side effects of treatment with this drug include heart and lung function issues, which need to be closely monitored in people taking this drug.
Not only do these results provide hope and more treatment options for patients with metastatic breast cancer, they will likely change the way we classify breast cancers by molecular subtype, adding HER2-low to the classification system. Ongoing clinical trials will test this drug on patients with different levels of HER2 expression to determine the range of expression that defines HER2-low tumors likely to respond.
To learn more about Trastuzumab Deruxtecan, visit the National Cancer Institute website. Click here for more information about breast cancer treatment clinical trials.
It’s the fifth day of National Breast Cancer Awareness Month 2022! Quick update from yesterday – my (hopefully) last breast reconstruction procedure went great! I’m home recuperating and enjoying love from my fur babies and my family. I haven’t looked at the result yet, but the left side of my surgical bra looks fuller. Hooray!
Now, back to the subject of breast cancer molecular subtypes! To recap, breast cancer isn’t a single disease. It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
Molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment, include four subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer TNBC.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about the triple negative subtype, which do not express hormone receptors for estrogen and progesterone and also do not express express a cell surface protein receptor called HER2. That’s how it got its name, triple negative, because of the three receptors it does not express. These breast cancers have other ways of growing abnormally that don’t involve hormones or HER2, and they tend to grow very fast. For example, some TNBCs have higher higher than normal levels of EGFR receptors, which are in the same cell surface receptor family as HER2. Like HER2, EGFR normally tell breast cells to grow during normal development in puberty. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Aside from targeting EGFR, a strategy being tested in clinical trials, people with TNBC have fewer treatment options with targeted therapies (therapies that inhibit hormone receptors and HER2) than other subtypes.
Aside from EGFR receptors, what make TNBC cells grow? There are several molecular pathways that become altered in TNBC. These pathways often function in normal breast epithelial cells telling them to grow when appropriate (cell surface receptors like EGFR, FGFR, and CSF1-R). When receptors on the surface of the cell becomes activated, they send signals to the breast cell that tells it to grow, like when your breasts are growing during puberty. Normally, after puberty, the receptor and related receptors are no longer activated and your breast cells stop growing. In breast cancer, your breast cells make too many receptors, which become constantly activated, making your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these receptors make the cancer cells grow uncontrollably.
One interesting characteristic of TNBC is that this subtype often has more interactions with the body’s immune system, meaning that immune cells travel to the tumor, get inside of it, and try to kill cancer cells and eliminate them from the body. Many cancer cells develop defenses against the immune system, using cell surface proteins like PD-1, PD-L1, and CTLA4 to shut down the immune cells. Tumors with lots of immune cells, called immunologically “hot,” may respond well to immune therapies that block the activity of PD-1, PD-L1, and CTLA4. The drug Pembrolizumab, which targets PD-1, is used to treat advanced TNBC. The drug Sacitiuzumab Govitecin was recently approved to treat TNBC. More on that below!
TNBC breast cancer is not as common as HR+ breast cancer, accounting for 15-20% of breast cancers. However, these breast cancers are often more aggressive and faster growing than HR+ breast cancer. They also disproportionately affect younger women and women of African descent. They are diagnosed by a pathologist based on analysis of gene and protein expression if ER, PR, and HER2 present in cancer cells in a biopsy and in the tumor after surgical removal. Low or no expression of these three receptors leads to a diagnosis of TNBC. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor.
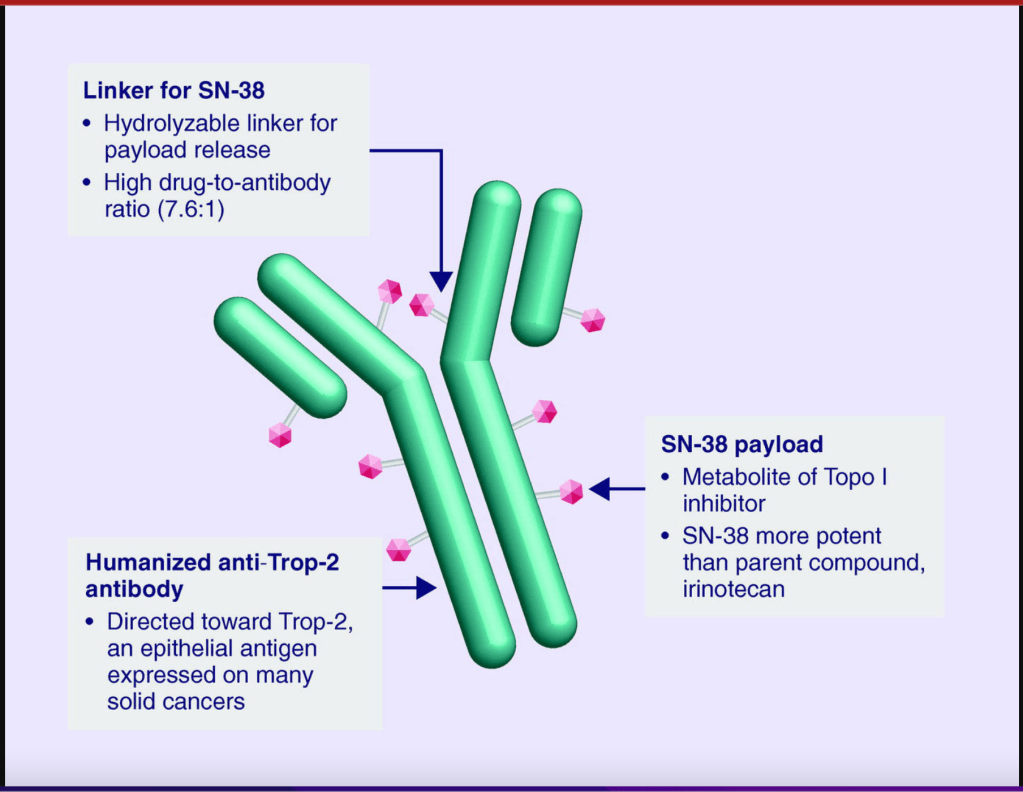
Follow-up treatments include chemotherapy, which was the only option for people diagnosed with TNBC for many decades. Recently, drugs developed specifically to treat TNBC have been approved and are being used in the clinic and undergoing additional testing in clinical trials to refine and optimize their ability to work with other drugs to kill more cancer cells. I discussed Pembrolizumab above. Let’s go over a little bit about Sacituzumab Govitecan. This drug binds to the cell surface protein Trop-2. Many TNBCs have higher than normal levels of Trop-2 on the surface of their cells. Sacituzumab Govitecan, approved in April of 2022, as a treatment for metastatic TNBC, is an antibody-drug conjugate that uses the an antibody against Trop-2 to carry a toxic drug directly to breast cancer cells with high levels ofTrop-2, targeting tumor cells and reducing damage to normal cells and tissues.
These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on TNBC, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams. Though TNBC is trickier to detect, screening mammography remains a vital tool for early detection of TNBC and other breast cancer cell types.
It’s the fourth day of National Breast Cancer Awareness Month 2022! Today, I’m undergoing my eighth breast surgery, seventh in a series of procedures related to cancer. In May of 2020 I had a single mastectomy to remove my left breast after we found residual cancer. In November of 2020, I began the process of reconstruction starting with a Diagonal Upper Gracilis (DUG) Flap procedure in which my surgeon removed tissue from my right thigh and grafted it to my chest, forming the foundation of a new breast, along with a reduction and lift of my right breast to start the process of making my boobs symmetrical.
It’s been a long, involved, two year process.
Part of the challenge is symmetry. Since I chose to keep my right breast, it’s harder to build a new breast with the same general size and shape. As one of the surgical residents once told me, they’re twins, but they’re going to be fraternal, not identical. I can live with that, especially since I can still feel and enjoy my right breast.
The quest for volume and symmetry has involved a series of fat grafts, transferring fat from my flank, left thigh, hips, and my back on this next round to my left breast. It’s working! Each time we get a little closer to a matching pair that look pretty freakin’ good. Yes, I have scars and always will, and yeah, my nipples point in different directions, but after the last procedure, I was comfortable in a T-shirt for the first time in since my mastectomy.
I’ll take it.
I’m going into this with a mixture of excitement and trepidation. Once again, I’ll be going under anesthesia and under the cannula if not the knife. I’ll be putting my body through the ringer again, going through the process of healing from wounds and bruises, both internal and external, as well as whatever psychological reaction I experience post-surgery. Bandages and binders, aches from having an IV needle jammed into my left hand as I cry silent tears and kick myself for doing this. I owe my body a big apology. I question my decision and wonder if its worth it.
Then, I take a deep breath and remind myself that I’m still here, surviving and thriving. Cancer took a lot out of me, but I won’t let it steal my joy or rob me of my resolve to get my body put back together in a way that works for me. At the end of the day, that’s what matters.
So, wish me luck, and I’ll see y’all on the other side!
It’s the third day of National Breast Cancer Awareness Month 2022! To recap, breast cancer isn’t a single disease. It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
Molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment, include four subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about the HER2-enriched (also called HER2+) subtypes, which express a cell surface protein receptor called HER2. These breast cancers have higher than normal levels of HER2 receptors, which normally tell breast cells to grow during normal development in puberty. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Luminal B breast cancers have too much of the cell surface receptor HER2 in addition to having too much estrogen and progesterone receptors (ER/PR +ve), as do breast cancers that do not also express hormone receptors (HER2-enriched).
How does HER2 receptors make breast cancer cells grow? When the receptor on the surface of the cell becomes activated, it sends a signal to the cell that tells it to grow, like when your breasts are growing during puberty. Normally, after puberty, the receptor and related receptors are no longer activated and your breast cells stop growing. In breast cancer, your breast cells make too many HER2 receptors, becoming constantly activated ,making your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these HER2 receptors make the cancer cells grow uncontrollably.
HER2+ breast cancer is not as common as HR+ breast cancer, accounting for 10-20% of breast cancers. However, these breast cancers are often more aggressive and faster growing than HR+ breast cancer. They are diagnosed by a pathologist based on analysis of HER2 gene expression and HER2 proteins present in cancer cells in a biopsy and in the tumor after surgical removal. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor. .
Follow-up treatments include chemotherapy andHER2-targeted therapies that block the activity of HER2 on breast cancer cells, including antibody drugs that bind to HER2 receptors and cause them to be degraded by the cell as well as triggering the body’s natural immune system to attack HER2+ tumor cells. These drugs include Trastuzumab and Pertuzumab. A derivative of Trastuzumab called Ado-trastuzumab emtansine (also called T-DM1) is an antibody-drug conjugate that uses the Trastuzumab antibody to carry emtansine chemotherapy directly to breast cancer cells with high levels of HER2, targeting tumor cells and reducing damage to normal cells and tissues.
These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on HER2+ positive breast cancer, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams.
It’s the second day of National Breast Cancer Awareness Month 2022! Did you know that breast cancer isn’t a single disease? It is a collection of diseases that cause cells in the breast—specifically the cells that produce and deliver milk to nursing infants called epithelial cells—to grow uncontrollably, forming a tumor. Each breast cancer case is as unique as each person, but they can be classified based on similarities in how they look under a microscope (histology) and on the characteristics of their DNA (molecular).
This post and upcoming posts will focus on molecular breast cancer subtypes, which are crucial diagnostic tools used to determine the best and most appropriate course of treatment. There are currently four molecular breast cancer subtypes recognized by scientists and clinicians based on their expression of hormone receptors (HR) for estrogen and progesterone (ER and PR) and their expression of the cell-surface receptor HER2: Luminal A, Luminal B, HER2-positive, and Triple Negative Breast Cancer.
ER = estrogen receptor, PR = progesterone receptor, HER2 = positive for the cell surface receptor HER2, Ki-67 = a marker for how fast cancer cells grow, -ve = negative, +ve = positive. Image Credit Here.
Today’s post is all about Luminal A and Luminal B subtypes, which are hormone receptor-dependent (hormone receptor-positive, also known as estrogen receptor-positive or estrogen receptor/progesterone receptor-positive). These breast cancers have higher than normal levels of receptors for estrogen (ER+) and progesterone (PR+), which normally tell breast cells to grow during pregnancy as they get ready to start producing milk. In cancer, these receptors stay active and make breast cells grow when they shouldn’t, which is a key characteristic of breast cancer. Luminal B breast cancers also have too much of the cell surface receptor HER2, which also makes breast cells grow uncontrollably, contributing to cancer. HER2 positive breast cancer will be covered in the next post.
How do estrogen and progesterone receptors make cancer cells grow? Estrogen produced by your body binds to molecules called receptors. When estrogen or progesterone enters a breast cell, it binds to a partner, called a receptor. When the receptor binds to the hormone, it sends a signal to the cell that tells it to grow, like when you’re pregnant and your breasts are getting ready to make milk for when the baby is born. Normally, after pregnancy and lactation, estrogen levels in your body go down and your breast cells stop growing. In breast cancer, your breast cells make too many receptors, so when estrogen levels go up in your body, like during your normal menstrual cycle, your breast cells grow abnormally, which is one hallmark of cancer. If other changes occur in your breast cells to form a cancerous growth, these estrogen and progesterone receptors make the cancer cells grow uncontrollably.
Hormone receptor positive, also referred to as ER+, ER/PR+ breast cancer, is the most common type of breast cancer, accounting for 70-80% of breast cancers. They are diagnosed by a pathologist based on analysis of hormone receptor proteins present in cancer cells in a biopsy and in the tumor after surgical removal. This type of breast cancer, like most breast cancers, is first treated by surgery to remove the tumor. Depending on stage and grade, the ER/PR+ breast cancers should be analyzed by tumor genomic tests like Oncotype Dx or MammaPrint, which helps predict how likely the cancer is to recur (i.e. come back) and if chemotherapy is necessary for treatment.
Follow-up treatments include hormone therapies that block the activity of estrogen in the body, like the drug Tamoxifen, drugs that block estrogen production by the body, aromatase inhibitors like Letrozole, Arimidex, and Exemestane, or drugs that degrade estrogen receptor like Fulvestrant. Other ER+ breast cancer treatments include drugs that block the activity of proteins that drive cell growth (CDK inhibitors), including Ribociclib, Palbociclib, and Abemaciclib. These are typically used in combination with endocrine therapies like Tamoxifen/AIs/Fulvestrant to treat metastatic breast cancer, which has spread to other parts of the body. For women diagnosed with cancer who haven’t yet undergone menopause, medically induced menopause may be recommended. These treatments reduce the risk of the cancer from coming back, or recurring. They do come with some not-so-great side effects, which your oncologist should consider and help you with. Quality of life should always be a consideration when it comes to cancer treatment.
For more on hormone receptor positive breast cancer, check out the American Cancer Association. As with other subtypes of breast cancer, early detection increases your chance of survival, so keep up with your routine mammograms and self-exams.
One of the things I love about my work in advocacy is discovering amazing people who are doing the work and making a difference! Valeda Keys is one such remarkable person. She’s a Global Ambassador for Breast Cancer Awareness, using her platform and the Non-Profit organization she founded, Valeda’s Hope, to assist women in their journey from diagnosis to remission. She has one hell of a compelling story that includes a family history of breast cancer, a personal battle with breast cancer that included seven surgeries, and finding strength and empowerment in helping others.
When I learned about her work on LinkedIn, I was blown away.
Valeda, who is an Author, Speaker, LPN, Non-Profit Founder, Breast Health Navigator, and all around incredible human being, helped her mother through a breast cancer diagnosis, treatment, and later recurrence. A dream told her that she would one day endure her own battle with breast cancer, which unfortunately came true in 2010. Luckily, because of her family history, Valeda started receiving mammography screening at the age of 27 and kept up with her screenings, which allowed her healthcare team to detect her first breast cancer at an early stage. After a lumpectomy, she received the results of her genetic testing, which revealed that she carries a variant of theBRCA-2(BReast CAncer gene 2) gene associated with an increased risk of breast and ovarian cancer.
Everyone has two BRCA1 and two BRCA2 genes, but sometimes a variant of one of these genes that doesn’t work gets passed down from one of your parents. If something happens to the other copy of the BRCA gene in a cell (for example, a cell from your breast or ovary), it can increase your risk for cancer. Why? BRCA genes encode information to make proteins that help fix damage to DNA. DNA molecules encode and store all the information a cell needs to make proteins, which allows a cell to live and perform its function. When DNA is damaged, it messes with the code, and if the damage isn’t repaired, cells make defective proteins that don’t function well or in the case of cancer-causing oncogenes, function too well. Defects in some genes make cells grow uncontrollably, and sometimes those cells turn into cancer cells. Variants of BRCA genes that don’t function to fix DNA damage makes it more likely for oncogenes to get activated and make cells grow uncontrollably, leading to cancer. In the graphic above, you can see a DNA repair deficient breast cell in which the BRCA genes encode DNA repair proteins that don’t work. Because the defective BRCA gene produces a defective protein, the cell can’t repair DNA damage and gets a lot more mutations in a lot of different genes. Some of these mutations create defective proteins that let the cell grow uncontrollably, even without estrogen (E2) or other cues from the body that tell cells when to grow. See my Cancer 101 blog post and my other blog poston how cells become cancerous for a refresher on the cell biology of breast cancer, DNA damage and how it leads to cancer, and oncogenes.
End Science Break
Now, back to Valeda’s story. Since she carries a variant of BRCA-2 that doesn’t work, she was still at risk for getting another breast cancer or ovarian cancer after her first breast cancer diagnosis. She decided to keep her breasts and get screened more often, a valid choice. (Note: there are no right or wrong choices when it comes to keeping your breasts or having a double mastectomy. There are only informed choices you make with your healthcare team that are right for you.). She also endured radiation therapy that led to some serious complications, and was treated with tamoxifen, a drug that blocks estrogen function. In spite of this, she was diagnosed with a new breast cancer in 2011 and opted for a double mastectomy and autologous reconstruction (i.e. reconstruction using her own tissue from her abdomen to build new breasts), which unfortunately came with some complications, and later had a hysterectomy.
Through it all, she remained focused and determined not to let breast cancer get in the way of living a full life and achieving her goals. Her faith helped her through, and it gave her a mission to educate, empower, and help other women through their own breast cancer journeys. Among the many amazing things she does through Valeda’s Hope, Valeda sponsors a ton of mobile mammography events and encourages women to keep up with life-saving screenings. She shares her knowledge and experience through speaking engagements and educational events like Valeda’s Hope Pink & Pearls Luncheons. Valeda also hosts events that provide emotional and physical support as well as information about genetic testing for breast cancer risk genes, and so much more.
A fantastic book by an amazing survivor!
I’ve said it before, and I’ll say it again: the breast cancer survivor community is so supportive! Survivors support other survivors, patients, and caregivers. As a survivor, Valeda is using her voice and actions to help other women survive and thrive, and that deserves a spotlight, kudos, and celebration!
It’s funny. I’ve been meaning to write more blog posts, but I’ve been so busy with work, family, writing, and…COVID. My whole family got the ‘Rona and it sucked. Fortunately, we’d been vaccinated, and my husband and I had been boosted. It didn’t result in hospitalization or death. We were lucky. My birth mother, Mary Etta Caldwell, was not. We lost her to Covid and I’m still reeling. PSA – the pandemic isn’t over. It’s still killing people. It’s still debilitating people with long haul Covid. Get vaxxed/boosted and stay safe out there.
Now, onto the main event. This one’s a fucking RIOT!!!
I don’t know if this was from a bot, but I’d like to think it’s from a man. I picture a middle-aged white man who is possibly unemployed and likes to slide into women’s DMs and make sexist comments, spew pseudoscience woo woo, and is a fan of Trumplican propaganda on Facebook and Twitter. We’ll call him Arthur – because that’s what his profile says!
Arthur is very concerned about me and my health. So concerned, in fact, that he reached out in a very sincere and grammatically sound Facebook Message to save me. Now, he hasn’t read my book—though he promises he will and I totally believe him—but he has vital information that he must share with me. Aren’t I lucky?
Arthur has the secret to cancer. Are y’all ready? It’s a dry rot fungus addicted to sugar, and all you need to kill it is hot water.
Straight out of my Facebook Messenger!
But if I REALLY want to keep the fungus at bay, I need to “maintain a LOW GLYCEMIC diett” and since “your carryinga little extra weight,” I must still be eating a high glycemic carb “amoint.”
Now, I’ve received flak before for pointing out bad grammar and spelling in personal attacks, but come on! This fucker reached out to me, a breast cancer survivor and researcher, with unsolicited advice and, quite frankly, the STUPIDEST explanation for cancer I’ve ever heard—and I’ve heard some real doozies.
But, beyond the poor grammar, spelling, and general stupidity, there is so much more fodder here for me to unpack. Firstly, mansplaining. It’s a thing. Ask any woman in your sphere and she’ll tell you. She won’t even have to think about it, and will probably come up with five personal experiences in less than a minute. I am an expert in the field of breast cancer. Not sort of, kind of, I guess I know a little—I’m a bona fide expert in the field with a Ph.D. and more than twenty years of experience studying the disease. I also have personally experienced breast cancer IN MY BODY. I know what I’m talking about, and the information I share is carefully researched and derived from peer-reviewed scientific publications.
And yet, like so many mediocre white male living examples of Dunning-Kruger, he just couldn’t help himself! Yes, I’m singling out white men. No, I don’t think it’s out of line. If you’re a white man and you’re offended, then you’re an Arthur and you need to rethink your life choices and behavior. If you’re not offended, you’re an ally and you should call out the Arthurs in your life because they’ll listen to you as a fellow white man. You can do it. It’s easy and fun.
Next, the fungus thing. I don’t think Arthur is giving white rot fungus a fair shake. Apparently, it is quite a useful organism that plays a vital role in the global carbon cycle by breaking down lignin, an organic polymer component of plant cell walls, especially in wood and bark, that lends rigidity and do not rot easily. If we didn’t have dry rot fungi, we’d have a whole lot of dead trees mucking up the planet.
But Dr. Dana, does it cause cancer??
Of course not!* In fact, an early pre-clinical study performed in colon cancer cell lines reported that extracts from a species of dry rot fungus, Cerrena unicolor, caused cancer cells to die in culture. That’s right, my friends. I think white rot fungi should sue Arthur for slander. Arthur is spreading malicious propaganda against this very useful organism that does more good on planet earth than Arthur could ever hope to achieve. Clearly, Arthur is jealous.
Now, as for sugar and cancer, it’s complicated. Biology is complicated. Anyone who says anything different is trying to sells you bullshit supplements. I wonder if Arthur sells supplements… Anyway, metabolism consists of a complex series of interconnected biochemical reactions that convert food energy into cellular energy required to fuel cellular processes, generate building blocks necessary to create/sustain/repair biomass, and eliminate cellular waste. Metabolism gets fucked up in very interesting ways in cancer cells and in the cells that surround it (microenvironment). Obesity is a metabolic health issue and a risk factor for breast cancer.
However, as noted by the American Cancer Society, “But the connection between weight and breast cancer risk is complicated. Studies suggest the risk appears to be increased for women who gained weight as an adult but may not be increased among those who have been overweight since childhood. Also, having extra fat in the waist area may raise risk more than having extra fat in the hips and thighs.” There are many, many dedicated, highly trained, competent scientists and physicians studying the complexities of metabolism, and there’s plenty they still don’t know.
I guarantee they know WAAAAAAAAAAAAY more about the subject than Arthur, who has no medical degree, no credentials, and no peer-reviewed studies to back up his assertions. The only thing he has is the audacity. As for the not-so-subtle dig on my weight, I can’t say it better than Lizzo. I’m a big bitch. I don’t have a tour bus, but I’ve got a degree, a platform, and I do a lot of good in the world. What do you do that’s worth anyone’s while, Arthur?
Lizzo is the undisputed QUEEN and I ADORE HER!
*If you want to hate on fungi linked to cancer, you should really go for Aspergillus flavus and Aspergillus parasiticus. They produce aflatoxins, and exposure to those increases liver cancer risk.
In summary, in a world full of Arthurs, be a Lizzo.
I was going to end it here, but Arthur slid back into my DMs to leave these little nuggets of wisdom:
From my Facebook Messenger – It’s an interesting place.
No, I’m not clicking on any of those links, because I don’t want a computer virus. Somehow, I don’t think this is the only virus Arthur is carrying. I hope you’ve found this post informative and entertaining, because I had a HOOT writing it! Thank you, Arthur.
Cancer is a great and terrible equalizer. It doesn’t care if you’re a Democrat, Republican, Independent, or if you support other political philosophies or are apolitical. Anyone can be diagnosed with cancer. For breast cancer, access to routine screening and diagnostic imaging is critical for early detection, accurate diagnosis, and receiving treatments in a timely fashion.
It can literally mean the difference between life and death.
When breast cancer metastasizes, or spreads to other parts of the body, time is precious, and people living with metastatic breast cancer need all the financial and medical support they can get.
How can you help? There are two pieces of legislation in need of support and a federal program in desperate need of reauthorization:
The first piece of legislation, the Access to Breast Cancer Diagnosis (ABCD) Act, will reduce out-of-pocket costs for diagnostic imaging for people with health insurance. While screening mammography is normally covered, additional imaging that’s needed when something suspicious or abnormal is spotted on a mammogram can become pricey. For each of my diagnoses (initial breast cancer diagnosis and diagnosis for residual disease), I required additional diagnostic mammography, diagnostic MRI, and diagnostic ultrasound. They were most DEFINITELY medically necessary to determine that the suspicious lesions on my mammography were indeed cancer – and for past follow-up diagnostic imaging, to determine that suspicious lesions were benign. This legislation will reduce the financial burden for diagnostic imaging that can be a barrier for early diagnosis.
The second piece of legislation, the Metastatic Breast Cancer Access to Care Act, would reduce wait times for receiving Social Security Disability Benefits and Medicare. Right now, the wait time for Medicare benefits for people living with metastatic breast cancer is 5 months, and the average wait for disability is 24 months. The five-year survival rate for stage 4 metastatic breast cancer (MBC) is 22 percent, and the median survival is three years (Reference). As one legislative staffer noted when I spoke with him about the issue and the wait times, “That’s cruel.” It is. People living with MBC need medical care coverage and financial support for themselves and their families. Legislation waiving wait times for ALS and end-stage kidney disease passed, setting a precedent for this important legislation supporting MBC.
Finally, reauthorization of the National Breast and Cervical Cancer Early Detection Program, will preserve and expand access to screening for un- and under-insured American. Early detection increases a patient’s chances of survival, so this life-saving program needs your support.
Please help these Bills become Law!
Please contact your Senators and Congressional Representative and urge them to co-sponsor and/or support these three key pieces of legislation. Feel free to copy and paste information from this blog post or use it as a script in a phone call.
The book has been out for about 3 weeks and I’ve been thrilled/nervous/pee-my-pants-excited to see my Amazon ranking as well as checking for ratings and reviews on Amazon, Goodreads, and other retail sites like Barnes & Noble, Walmart, Google Books, and Rowman & Littlefield!
For a brief, beautiful, shining moment, it was the #1 New Release in Breast Cancer and Oncology on Amazon, and I have the screenshots to commemorate it!
Pics or it didn’t happen!
Want a sneak peek? Of course you do! Here’s an excerpt from Chapter 16 that deals with an exciting new development in cancer research and treatment – harnessing the patient’s own immune system to seek out and destroy cancer cells through immune checkpoint inhibitors.
EXCERPT
I’ll also take comfort in the fact that we’re getting new weapons in the arsenal for fighting breast cancer. Antitumor immunity is the hottest thing to hit the field of cancer research since the 2001 approval of Gleevec (a game-changer drug used to treat chronic myelogenous leukemia that targets the oncoprotein product of the Philadelphia chromosome that drives the disease) and the 2006 approval of Gardasil (first vaccine targeting the human papilloma virus strains that cause most cervical cancers). Recently Frontiers in Immunology published the history of antitumor immunity efforts leading to the development of immune-checkpoint inhibitors available in the clinic today, the use of engineered T-cells taken from patients and altered to fight their cancer, and oncolytic viruses.2 I’ll go over the basics, including how antitumor immunity works and the challenges we still face in getting tumors to respond.
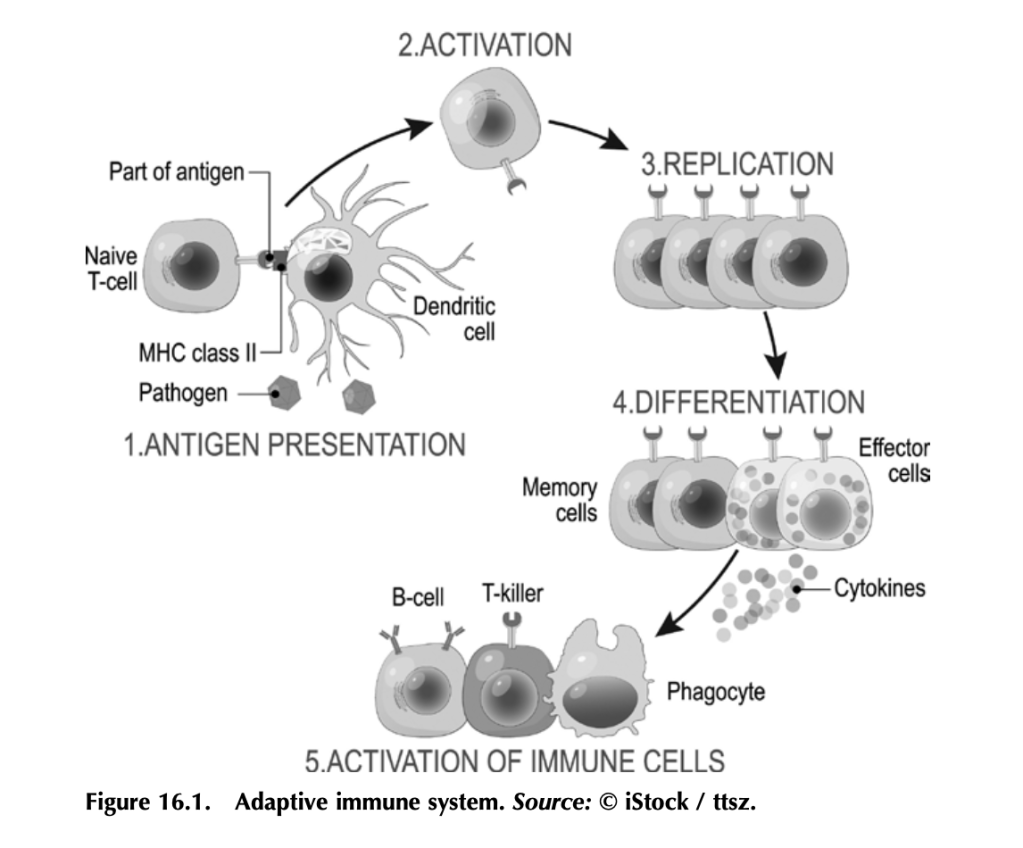
Before we get into how antitumor immunity works, we need to understand how the immune system works to fight infection. It’s a complex beast, but here are some basics. Your immune system functions to mount a rapid and robust defense when your body encounters a pathogen (e.g., a virus or bacteria that causes disease) in your daily life. The arm of the immune system that does this is called the adaptive immune system (figure 16.1). The other arm is the innate immune system, which includes natural barriers like skin, the tiny hairs and mucous in your nose, and stomach acid. The adaptive immune system is what antitumor immunity treatments harness. It is also altered by tumors to suppress tumor immune responses and exploited to work for the tumor. (More on that in a bit.)
The adaptive immune system works like this: Specialized cells identify a potential threat (e.g., an infection), and they carry information about that threat in the form of bits of protein called antigens to other immune cells. If the threat is credible, those immune cells get activated and fight the threat. First the specialized cells that identify a potential threat patrol your body, looking for something suspicious. Cells like macrophages and dendritic cells, which roam around various organs and tissues, find pathogens (a bacteria, virus, or other microbe that causes disease) or unhealthy cells infected by pathogens, and eat them (the fancy term is phagocytosis). Infected or damaged cells send out protein signals called cytokines as a distress call to attract these patrolling macrophages and dendritic cells. While “digesting” the bacteria or infected cell, macrophages and dendritic cells salvage proteins or pieces of proteins—antigens—that identify the bacteria or virus as “other,” and they present these to immune cells, usually in lymph nodes, which in turn mount an immune response. Macrophages and dendritic cells are known as professional antigen presenting cells (APCs).
When activated by APCs, immune cells called B-cells produce antibodies against the antigen, which can do a lot of things to fight an infection. Some antibodies neutralize the pathogen by binding it and stopping it from entering a cell. Other antibodies tag infected cells as a signal for other immune cells to come and kill them. Others coat pathogens or infected cells in a process called opsonization (meaning “the process of making tasty”), which signals other cells like macrophages to come and eat the coated pathogens or cells. Specialized B-cells called memory B-cells store the information about the antigen so your immune system can recognize the pathogen when it hits you again and mount a faster immune response.
Other immune cells called T-cells, which are particularly relevant to antitumor immunity, become activated by APCs and mount a different kind of immune response. Cytotoxic T-cells seek out and kill infected or damaged cells, and helper T-cells help activate B-cells so they make antibodies, activate cytotoxic T-cells, and activate macrophages to go eat nasty invaders and infected cells. Memory T-cells also store information about past infections to mount a rapid, strong response the next time your body sees it.
That’s a simplified but hopefully digestible explanation of immunity and the major players (there are other immune cells, but APCs, B-cells, and T-cells are the biggies).
Memory is key to protection, and memory is built by exposure to pathogens.
Put a pin in that concept for when we get to anticancer vaccines, and also remember what T-cells do for when we get to engineered CAR T-cells and oncolytic viruses.
Working out how to harness your body’s own immune system to fight cancer isn’t a new idea. It’s been under investigation since the nineteenth century. In fact, in chapter 5 we covered the way trastuzumab (trade name Herceptin), a humanized anti-HER2 antibody, targets HER2-expressing breast cancer cells for death. Herceptin and other monoclonal antibodies mimic the natural activity of antibody- producing B-cells to deliver therapies and tag cancer antigen–expressing cells for immune-mediated destruction. But it was the discovery of checkpoint inhibitors—proteins that put T-cells in a state of exhaustion and inactivity in pathways that are exploited by many cancers— that led to the first molecularly targeted therapies designed to boost antitumor immunity. Doctors James Allison and Tasuku Honjo pioneered this Nobel Prize–winning work.3
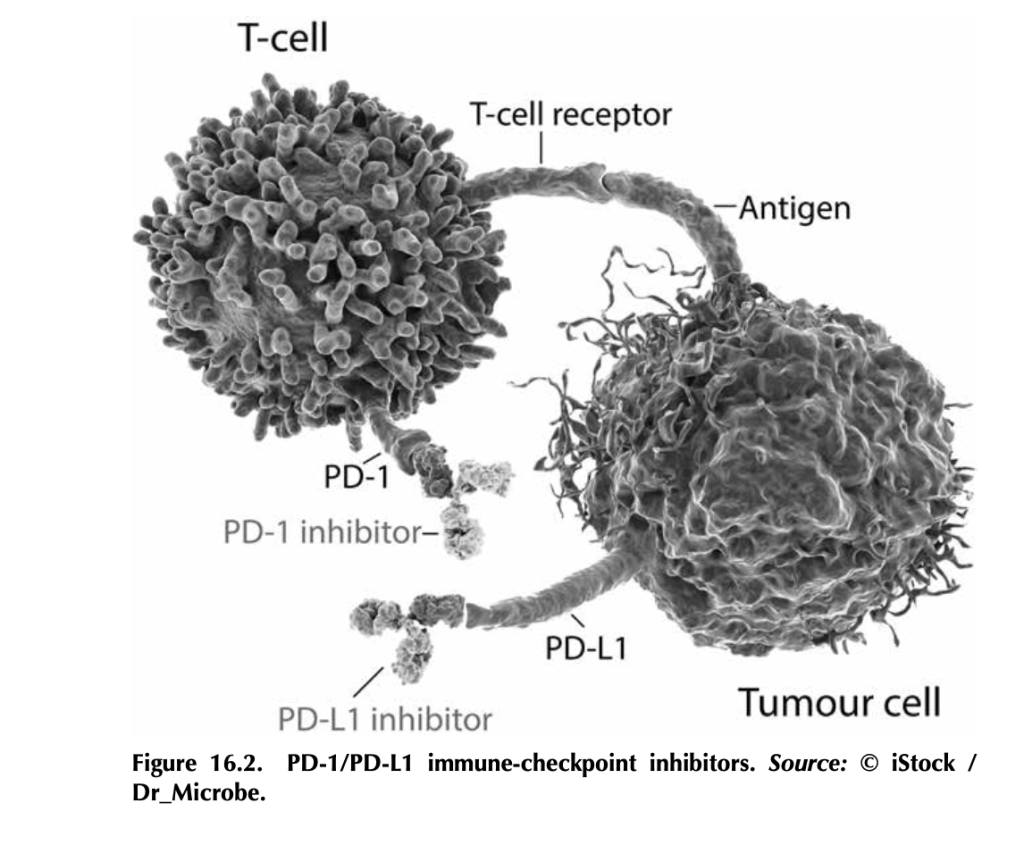
What are immune-checkpoint inhibitors, and how do they work? T- cells, particularly cytotoxic T-cells that actively kill their targets, bind to antigens on tumor cells through their T-cell receptors. But tumor cells, being the adaptable beasts that they are, can produce proteins like PD-L1 (programmed death ligand 1), which bind to PD-1 (programmed cell death protein 1), proteins on T-cells. This interaction tells the T- cell to stand down by tricking it into thinking that the tumor cell is “self” and should be protected. Signaling networks like this normally promote self-tolerance so that your immune system doesn’t attack your own healthy cells (figure 16.2). In tumors, it works by telling tumor- infiltrating T-cells, if present, to go into a state of inactivity. Drugs that target PD-L1—like atezolizumab (trade name Tecentriq), durvalumab (trade name Imfinzi), and avelumab (trade name Bavencio)—and drugs that target PD-1—like nivolumab (trade name Opdivo) and pembrozolimuab (trade name Keytruda)—are FDA-approved mono- clonal-antibody therapies that block interactions between PD-1/PD-L1 to unleash an antitumor immune response.4
Other immune-checkpoint molecules exploited by cancers include cytotoxic T lymphocyte antigen 4 (CTLA-4), the target of the first FDA-approved immune-checkpoint inhibitor ipilimumab (trade name Yervoy). Approved in 2011 for advanced melanoma, this drug had remarkable results. In fact, over 20 percent of the patients enrolled in the initial ipilimumab clinical trials (before the 2011 approval) are still alive and show no evidence of disease (NED).
There’s some incredible potential in targeting checkpoint inhibitors.
CTLA-4 is part of a cellular-signaling pathway that normally fine- tunes immune responses. CTLA-4 and a similar receptor, CD28, are expressed on two different T-cell types: (1) CD4+ helper T-cells, which help activate other immune cells to mediate adaptive immune responses, and (2) CD8+ cytotoxic T-cells, those cells that kill infected cells, damaged cells, and, if properly activated, tumor cells. Antigen- presenting cells make a protein called B7, which can bind to either CD28 or CTLA-4 on T-cells, and the effects on T-cell function are very different depending on what B7 binds. If it binds to CD28, B7 activates T-cell responses as a part of a complex of proteins that includes the T-cell receptor. Binding of B7 to CTLA-4 shuts down T- cell functions. CTLA-4 probably serves as protection from self-antigen recognition by inducing immune suppression, since laboratory mouse models engineered to not express CTLA-4 die from autoimmunity. This is the aspect of CTLA-4 function that gets highjacked by tumor cells. Drugs like ipilimumab block the suppressive activity of CTLA-4, which can allow T-cells to attack tumor cells.5
Here’s the kicker: The tumor actually has to have infiltrating T-cells for this to work, and not all tumors do. Tumors with T-cells that can be activated to fight the tumor are called “hot,” whereas tumors without T-cells are “cold.” One of the most aggressively researched topics in tumor immunology right now is how to make a cold tumor hot and thus responsive to antitumor immune therapies.
This is especially important for breast cancer, since most subtypes produce cold tumors. Right now, immune-checkpoint therapies are only approved for advanced triple-negative breast cancers that make the PD-L1 protein. Not all triple-negative breast cancers make PD-L1. Ongoing research is looking to expand the use of immune therapy in inflammatory breast cancer and the HER2+ subtype.6 Hopefully, with more research, we’ll figure out how to make more tumors responsive to immune therapy by making them hot (full of T-cells) and by discover- ing other immune checkpoints that can be targeted.
3. Heidi Ledford, Holly Else, and Matthew Warren, “Cancer Immunologists Scoop Medicine Nobel Prize,” Nature, October 1, 2018, https://www.nature. com/articles/d41586-018-06751-0.
4. See American Cancer Society medical and editorial content team, “Immunotherapy for Breast Cancer,” Treating Breast Cancer, American Cancer Society, Cancer.org, last revised December 3, 2020, https://www.cancer.org/ cancer/breast-cancer/treatment/immunotherapy.html.
6. Devon Carter, “Does Immunotherapy Treat Breast Cancer?” MD Anderson Center (website), University of Texas, March 26, 2021, https://www .mdanderson.org/cancerwise/does-immunotherapy-treat-breast-cancer.h00 -159385101.html.
It’s been a while. This is my first post for Breast Cancer Awareness Month 2021, but I promise I’ve been busy in the laboratory. In the past two months, I’ve submitted grant applications to Breast Cancer Alliance, METAvivor, and Department of Defense CDMRP Breast Cancer Research Program. The first two are foundations that fund novel research projects, supporting scientists like me so we can take a chance on new projects that are higher risk/high reward and generate preliminary data for larger funding proposals. DOD supports larger research projects at both early (Breakthrough Level 1) and later (Breakthrough Level 2) stages. Fingers and toes crossed for grant funding! If you’re looking for organizations to support, I highly recommend Breast Cancer Alliance and METAvivor.
For this post, I’d like to highlight some survivor communities that have helped me and continue to help me, and to encourage patients and survivors to reach out for support. Cancer made me feel powerless. Sure, I was taking care of myself and following instructions from my surgeons, oncologist, and other providers, but they were doing things to me and for me – cutting out the cancer, managing my followup therapies, monitoring me to make sure the cancer wasn’t back, but I felt like I wasn’t (or couldn’t) do anything. That’s part of the reason I wrote Talking To My Tatas and why I started this blog. I needed to DO something.
I also needed to know I wasn’t alone. Enter other breast cancer patients and survivors. These people are some of the most generous human beings, providing support, practical advice, sharing their stories, and giving lots and lots of love to people who join this club we never wanted to be a part of but is filled with survivors in every sense of the word.
Where can you find support? Plenty of places! The Internet can be a terrible and wonderful place, and in the case of support for cancer patients and survivors, it can be a lifeline. Here are some survivor communities who’ve helped see me through on Facebook:
This is a large FB group dedicated to shared experiences and full of practical advice! I went to them when I was preparing for my mastectomy and I got a TON of tips for what to expect, what to stock up on (soft cotton camis and cardigans with pockets for surgical drains, pillows, etc.). Need advice from folks who’ve been there? Need to vent? Looking for hope? A safe place to express yourself? This is a great one!
Laughter is one of the best weapons we have when it comes to cancer, and you’ll get plenty of laughs from this group. Lots of boob humor. Check them out!
Want to know about the latest research? Looking to connect with survivors and get involved in advocacy, or do you need information on resources from financial to physical and mental health? This group is a great place to start.
Looking for a support community that welcomes patients and survivors outside of majority faith communities? This one is super helpful and supportive!
Not big on social media? Ask about support groups available through your medical center. Check out your local Gilda’s Club – just be sure to follow safety guidelines for Covid-19. Need a support community for African American breast cancer patients and survivors? Check out Sisters Network – they provide a space for African American breast cancer patients to meet, bond, and receive support during treatments. Similar organizations tailored to the unique needs and experiences of other communities of color include: The Latino Cancer Institute, The American Indian Cancer Foundation, and The Asian American Cancer Support Network. Support for LGBTQIA+ cancer patients, including a directory for LGBT-friendly cancer treatment facilities, can be found at The National LGBT Cancer Network.
No matter your background, culture, or identity, you don’t have to go it alone when it comes to breast cancer. I encourage you to find your support network and lean on them. And, when you’re ready, be a part of that community and give your support to someone in need.