When you’re diagnosed with breast cancer, no matter what stage or subtype, odds are you’ll be looking at surgery as part of your treatment plan. Got a tumor in your boob? Gotta have it cut out. Thankfully, patients have options when it comes to surgery, and, this is important…
THERE ARE NO RIGHT OR WRONG CHOICES – ONLY INFORMED CHOICES.
Whew, now that I got that off my chest (see what I did there?), let’s talk about two of those surgical options: lumpectomy and mastectomy (single mastectomy in my case, though many women opt for a double mastectomy and that’s okay). A lumpectomy involves removal of the tumor and surrounding tissue while preserving the rest of the natural breast tissue. A mastectomy is complete removal of breast tissue, leaving only skin and the underlying chest muscle behind. I’ve had both, so I speak from personal experience as well as through the lens of science. Here’s the scoop:
In 2018, I opted for a large lumpectomy followed by oncoplastic reconstruction. I’ll blog more about reconstruction options later, but oncoplasty refers to a breast reduction and lift. My tumors were small, I was early stage, and was a great candidate for this less invasive, breast conserving surgery. Even though I was later diagnosed with residual disease, I regret nothing. I simply got unlucky, and mastectomy was always an option if I had recurrence just as it was an option when I was diagnosed with residual disease.
In 2020, when we detected a pesky little 6 mm tumor that didn’t show up the first time, I opted for a mastectomy for the left breast. I chose this so I could maintain sensation on my right side. This was a personal choice – again, no right or wrong choices, only informed choices. I have the same risk of developing cancer in the right breast as I always had (no additional risk by having it in my left breast), and for me, being able to feel touch on the right side was important. Plus, as this 2017 article notes, “Contralateral prophylactic mastectomy (taking off both breasts including the one without cancer) is becoming increasingly common in the United States, and patients considering this option must be counseled about its lack of a survival benefit, its higher complication rate, and the fact that it is risk-reducing but not risk-eliminating.”
Before getting into the nuts and bolts, what are the outcome data for lumpectomy versus mastectomy? Breastcancer.org cites a 2014 article from JAMA Surgery, summarizing the data as follows:

When combined with radiation, patients who opted for lumpectomy had outcomes that were comparable (even slightly better on average) than patients who opted for mastectomy. Bottom line – for early stage disease, outcomes are comparable for breast conserving surgery versus breast removal.
*Disclaimer – ALWAYS ask your doctor about outcomes and survival odds for your specific breast cancer type, stage, and grade.
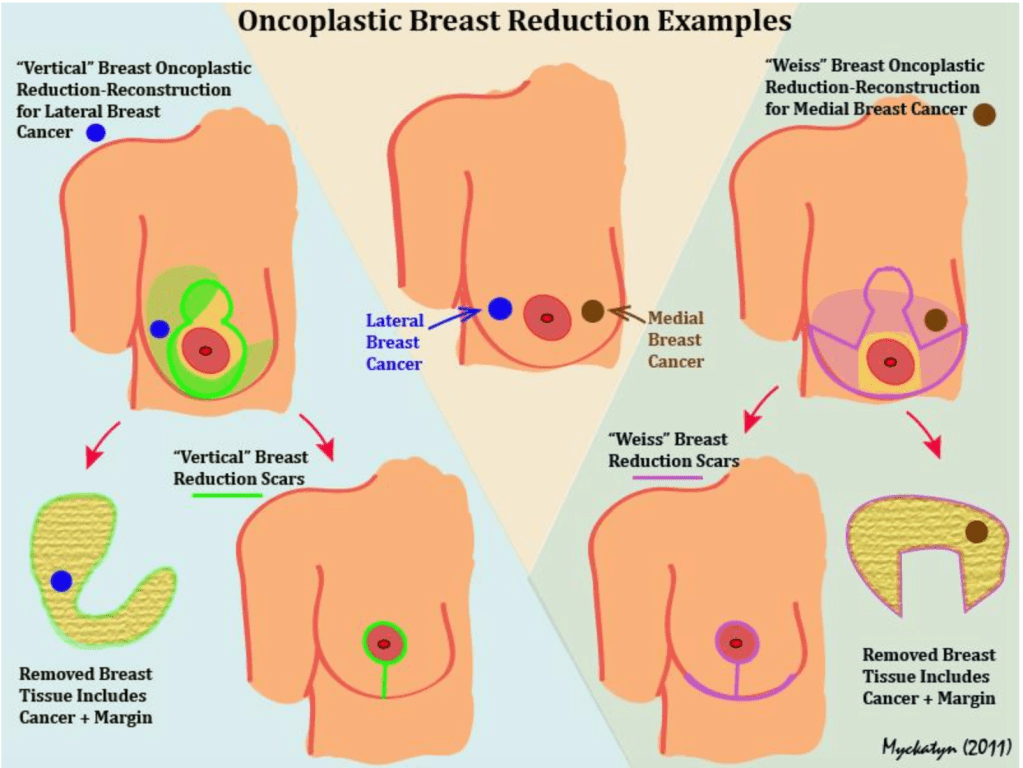
For the lumpectomy, my surgeon removed my tumors and surrounding tissue. Before that, my tumors were marked with Savi Scout devices, radar locators inserted into my left breast with GIANT FUCKING NEEDLES THE SIZE OF SCREWDRIVERS WHILE MY LEFT BOOB WAS IN MAMMOGRAM COMPRESSION. Yes, this is horrifying, but it’s waaaaay better than wire localization, having ACTUAL WIRES STICKING OUT OF YOUR BOOBS to help the surgeon find the target area. After my breast cancer surgeon cut out the tumor, my plastic surgeon took over to perform a reduction (cutting out tissue on both sides) and lift (cutting around my nipples and jacking them up along with the attached breast tissue and stitching the whole thing up in what I like to call an “anchors away” pattern.

For my mastectomy, which was a skin and nipple-sparing procedure, my surgeon cut out all of my breast tissue except for a small portion underneath the skin that contains blood vessels necessary to sustain the remaining skin. The point is to de-epithelialize (fancy term for getting rid of the glandular epithelium that is the source of breast cancer) the tissue to make sure no cancer/pre-cancerous cells are left in the chest area. In many cases, including mine, a tissue expander was implanted between the remaining skin and my chest muscle. After recovery and removal of surgical drains (see below), you go to your plastic surgeon’s office to have a nurse locate the built in port with a magnetic port finder and then stick a GIANT FUCKING NEEDLE into the port to fill it up with saline solution, stretching your skin in preparation for reconstruction. After the final fill, you have to wait THREE MONTHS with a HELLA UNCOMFORTABLE foreign body in your chest before reconstruction. That’s where I’m at right now – waiting for my surgery date.
Pros and cons? If you opt for mastectomy, you can most likely skip post surgical radiation therapy. Radiation therapy sucks! It’s painful, causes fatigue, and it takes several months to fully recover. If you opt for a lumpectomy, your surgical recovery time is much faster! I was up and about within 2-3 weeks after lumpectomy/oncoplastic reconstruction. For my mastectomy on the left side, I was down for the count for 6 weeks and not really back to myself until after 8 weeks and completing physical therapy (didn’t need PT with lumpectomy – another advantage). For lumpectomy, I was able to maintain sensation in both breasts/nipples. I could even still feel the one that got nuked (i.e. radiation therapy). For my mastectomy, sensation on the left side is all gone and most likely will never return. Lumpectomy followed by oncoplastic reconstruction gave me a great shape and aesthetic result. My tits were GORGEOUS (as a part of the reconstruction process, I had a reduction and lift on the right breast in order to achieve symmetry)! I went from saggy D cups to very perky, pretty C cups. It was like being 18 again! But, even though the odds were low, I was one of the unlucky patients who had residual disease following lumpectomy and radiation.

Another consideration – mastectomy required surgical drains. With the removal of tissue and damage resulting from cutting into the body, fluid accumulates in the wounded area and, if undrained, can result in a seroma. To mitigate this complication, the surgeon leaves plastic tubes in the area attached to external suction devices that look like grenades and that need to be emptied several times a day. What comes out ranges from pale liquid to blood red liquid to what I can only describe as “chunky salsa” as pieces of tissue drain out and can sometimes clog the drain and/or the bulb. Yes, it’s that gross. These drains can stay in for up to two weeks, making it impossible to shower, bathe comfortably, exercise, and otherwise operate like a normal, functional human being.
Okay, you CAN function normally, but you’ll fucking pay for it when your drains start filling up faster with bloody, chunky salsa because you overdid it, dumbass. Yeah, I was a total dumbass because “the rules don’t apply to me.”
The rules totally apply to me. Chunky. Salsa.

And, as noted. spending a minimum of three months with one or two expanders in your body following a mastectomy is a level of sucktastic that I can only describe as follows: I’m kinda like a femebot but without the cool guns. I mean, if you’re going to be a cyborg, you should at least get some cool powers, right? That’s a BIG con when it comes to mastectomy. My oncoplastic reconstruction for lumpectomy happened immediately after my tumor removal surgery, which was super efficient and came with a relatively easy recovery.
Bottom line (louder, for the folks in the back): THERE ARE NO RIGHT OR WRONG CHOICES – ONLY INFORMED CHOICES. Knowledge is power. Get as much information from your healthcare team as possible. Ask questions. Do your research (using reputable sources that cite peer-reviewed data). Ask more questions. You are your own best advocate!




