It’s day 23 of National Breast Cancer Awareness Month! I skipped a few days due to lack of spoons (see my previous post about spoon theory and chronic illness), but I have some extras today and am excited at the prospect of bringing my message to folks in Tampa, Florida, and beyond!
My amazing Literary Agent, Barbara Rosenberg, put me in touch with Linda Hurtado, an award-winning news anchor by day who writes heart stopping thrillers as Linda Bond (and I totally recommend checking out her books!). Linda then invited me to appear on her live show for Breast Cancer Awareness Month! It’s scheduled for Wednesday, October 26, at 12:00 pm EST for her Tampa Bay Reads segment. I’ll be talking about breast cancer from both a patient and research perspective, talking about the book, and hopefully convincing viewers to schedule their mammograms!
This will be my first television appearance and I’m both excited and a little nervous, but I have faith in Linda and I’ll just be prepared to be poised but still be myself as I share my story and hopefully some more information about breast cancer that the public needs to know.
Super grateful for the opportunity and hope it helps me make a difference! Wish me luck!
I’ll be sure to post the link in a future blog post!
It’s Day 20 of National Breast Cancer Awareness Month! Recovery from surgery is a funny thing. One the one hand, I have Wolverine-like powers in terms of physical healing. Most of the time. Except for those days when I’m in a funk. Those days when it’s hard to get out of bed, but I can’t sleep. Or I start falling asleep at my desk and get into bed, but can’t go to sleep there. When I’m excited to do something and then, when it’s time, find myself too fatigued mentally and/or physically to do the thing.
Which makes me sadder. And more fatigued. And it’s harder to get up the next time until and unless I force myself. But I pay for that with interest.
Fatigue, physical, mental, or the horrible double whammy of both at the same time, really and truly sucks donkey balls.
Spoon Theory is a metaphor for illness – originally chronic illness in the form of lupus and then expanded to include mental illnesses like anxiety and depression. It holds that healthy people have an unlimited amount of spoons, or possibilities, or energy—a form of currency—to accomplish their daily tasks with plenty left over for fun. With chronic illness or mental illness, your currency is limited. You don’t have as many spoons. So you have to budget. And you many only have enough spoons one day to shower. Or maybe you can shower and go to work, but you don’t have enough spoons to come home and make dinner or go out with friends.
Some days, you don’t have enough spoons to get out of bed.
Christine Miserandino, who came up with this brilliant analogy, explains it much better and you should totally grab a copy of But You Don’t Look Sick: The Real Life Adventures of Fibro Bitches, Lupus Warriors, and Other Superheroes Battling Invisible Illness to learn more, but that’s where I’ve been for the past several days. I have a friend who has fibromyalgia and other friends who have chronic illnesses who deal with this more than I do, though they still consider me a “Spoonie.” One of those friends once looked at me a few years after my 3rd or 4th cancer surgery and told me I was running myself ragged and was in danger of collecting another chronic illness and, as a result, losing more of my daily ration of spoons.
That hit me HARD. I was and still am a doer, a mover, a shaker. I walk fast. I’m always busy. I get shit done.
I still can, but not at the expense of my precious spoons. So, for the past two days, I’ve spent a lot of time in bed (going to bed early, napping, resting my eyes on the couch) and struggling to not beat myself up for it. It’s okay. Things will get done eventually. The important things. When I have more spoons.
So, dear readers, don’t beat yourselves up. Save yourselves. And your spoons. You’re worth it.
It’s day 19 of National Breast Cancer Awareness Month! Day 18 was super busy for me with work, doc appointments, and life, so I was unable to post. It happens. But hopefully today’s (late) post will be informative and eye-opening. It certainly was for me.
Sexism, racism, anti-Semitism, homophobia, and all the other prejudices and bigotries that plague humanity exist in science. On the one hand, scientists are rational people who should be objective, but on the other hand, scientists are, well, human. We’re not immune to biases and the cultural and societal systems in which we exist.
British physicist, Dr. Jess Wade, was reminded of this when she created a biography for prominent climate scientist Dr. Kim Cobb, discovering that deserving women like Cobb whose names — and lengthy list of achievements — had not been curated Wikipedia, the go-to site for most folks seeking information on the Internet. Naturally, male scientists do not suffer from the same issues and are often credited for achievements at the expense of female colleagues.
Google Dr. Rosalind Franklin and find out how bigot and all-around horrible human being James Watson stole her data and got credit for “discovering” DNA. He’s so bad he was stripped of honorifics after making bigoted comments about race and intelligence. Look up Dr. Arthur Eichengrün and find out how the precursor to the company Bayer, who collaborated with Nazis, gave credit for the discovery of aspirin to Dr. Eichengrün’s non-Jewish technician because of anti-Semitism and STILL haven’t acknowledged Eichengrün’s contribution. Yuck. I was today years old when I learned about Dr. Sophia B. Jones, the first Black female graduate of the University of Michigan’s Medical School in 1885 and later became the first female faculty member at Spelman College and spearheaded public health programs and health equity initiatives for Black Americans. There are countless other stories we’ve never heard of because of white supremacy and patriarchy, which celebrates the achievements of straight cis white males and minimizes or erases all others.
Dr. Wade decided to address this disparity by writing over 1,750 Wikipedia pages for female and minority scientists who didn’t already have their accomplishments documented on the site. Check out her own Wiki page, too! Not all heroes wear capes – some wear lab coats and cool glasses.
I’m totally going to make a Wikipedia page for myself. Men do it all the time, so why not??
Shout out to Dr. Wade, to the people behind these stories and their amazing contributions to science, and to a future in which we trade bias and bigotry for inclusiveness and giving credit where credit is due to everyone!
Thanks to my gal pal Florence Cardon for sharing the Washington Post article link with me, and to TikTok creator @inevitablebetrayal for shining a light on Bayer.
It’s day 17 of National Breast Cancer Awareness Month! Today’s post is all about celebrating our pet pals and how they support and heal us when we have cancer. I’m a lifelong cat fanatic. My first pet was a ginger tomcat who chased me through the house and yard and then curled up with me for a well-earned nap. I’ve been hooked ever since. Cats are wildly entertaining goofballs that toe the line between completely endearing and completely annoying, and I’m here for it!
Enjoy these goofy cats!
I am currently owned by three cats.
Vanilla (full name Vanilla Wafter Sieders Asshole IV), my son’s 5 year old Siamese who is gorgeous, had the biggest and best purrs, likes to give love bites and has a weird foot fetish. Then there’s Kuro (Kuro I’m the Good One Sieders), my daughter’s 4 year old black beauty who is a world class snuggler, has the sweetest purr, and turns into a ninja assassin when it’s time to trim her claws. Finally, my black cat (pandemic pet) Sheila (Sheila Bad Bitch Sieders) is 2 years old, gorgeous, dumb as a bag of rocks, and wildly entertaining. She also meows loudly and nonstop.
Vanilla looking distinguished and handsome in his winter holiday bowtie collar.
Aside from their many and varied personality quirks, whenever someone in the family is sick or recovering from illness (in my case, multiple surgeries and radiation therapy), the cats are on that someone 24/7, working in shifts to provide comfort and company. Kuro takes on the brunt of the work, curled up in a lap or on a chest with soothing purrs and comforting warmth, letting us stroke her silky soft fur and relax into her calm.
Kuro sitting on my lap (covered by her favorite soft blanket) in my home office. Yes, that’s a ceramic skull on my desk. And a hand-painted ceramic mermaid. And a “Donut Give Up” plaque. Don’t worry about it.
Vanilla will then take over, making biscuits on the blanket, purring, and demanding pets. He’s not big on cuddles, but he likes to sit close and slow blink. He’s 15 pounds of fluff and squishy love.
Sheila is not best pleased to be at the vet and is trying her best to hide behind my daughter.
Then, there’s Sheila. She’s a noodle of a cat, slinky and svelte, acrobatic, energetic, and adorable with her single braincell. She’s young, very busy playing and getting into all kinds of cat shenanigans, and always makes me laugh. She’s not often cuddly, but when she is, she melts. Her purrs are soft and subtle, and her fur is as sleek as she is.
I’m a believer in the healing power of cats, but what is the scientific evidence? Turns out, the emotional support benefits of pets for cancer patients are supported by the American Cancer Society and by a recently published literature review. Click on the links for tips to stay safe and healthy with pets while undergoing cancer treatments.
As long as your healthcare provider gives you the green light and you take precautions to protect yourself and your pets during treatment, take all the fur baby love you can get!
It’s Day 16 of National Breast Cancer Awareness Month! Today’s topic will cover one of the oldest targeted breast cancer drugs developed that is still used in the clinic today—tamoxifen. I’ve been taking it for 3 1/2 years, and millions of other breast cancer survivors with ER+ breast cancer have taken this drug as part of their treatments to prevent recurrence. But how was it discovered? How does it work?
Like many scientific discoveries, the discovery of tamoxifen was an accident. ICI46,474, later named tamoxifen, was first synthesized in 1966 by scientists working for a company that would become AstraZeneca. The goal of the project was to find a new chemical compound that could be made into a birth control drug. Laboratory studies were promising, but they found it didn’t work as a form of contraception in humans. This could have been the end of the story for tamoxifen, but one of the members of the team thought it might work as a breast cancer drug. In 1971, tamoxifen was tested in a clinical trial conducted in the UK on “late or recurrent carcinoma of the breast.” Thankfully, it worked!
How does it work? Since it started out as a candidate contraceptive, it makes sense that it was designed to block estrogen, a female hormone that helps prepare the uterus and uterine lining for pregnancy. It is in a class of drugs known as Selective Estrogen Receptor Modulators (SERMs), which are compounds that compete with the hormone estrogen for binding to its receptor. Normally, when estrogen binds to its receptor in the body, it triggers processes in the cell that make it divide, or produce more cells. This is called proliferation. In cancers with too many estrogen receptors (ER), estrogen in the body makes these cells grow uncontrollably. By binding to estrogen receptors in breast cancer cells, tamoxifen blocks this action and stops breast cancer cells from growing.
Around 70-80% of breast cancers are ER+, meaning that abnormal estrogen receptor activation is a key driver for growth of the breast cancer cells. Tamoxifen was a game changer for women with ER+ disease, reducing the annual breast cancer death rate by 31%. There are other drugs on the market that also block the activity of estrogen or downstream molecules in the estrogen receptor pathway, but tamoxifen remains standard of care for many cases of ER+ breast cancer.
As with any medication, tamoxifen comes with side effects that include: hot flashes, vaginal discharge, nausea, mood swings, fatigue, depression, hair thinning, constipation, loss of libido, dry skin. I experienced hot flashes, vaginal dryness and libido issues, and hair thinning, but they were not as severe as those I experienced with other estrogen blockers (aromatase inhibitors). For me, tamoxifen is a better balance between protection from recurrence and quality of life, but everyone’s physiology and experiences are different.
Be sure to talk to your healthcare providers about any side effects you experience. You don’t have to suffer in silence, and there are options to reduce side effects and improve your quality of life.
It’s day 15 of National Breast Cancer Awareness Month, and WHAT A DAY! There is something truly magical, beautiful, and inspiring about being surrounded by a crowd of survivors, their loved ones, and those devoted to the mission of ending breast cancer! Here are some highlights from today!
Shout out to our AMAZING volunteers who organized the event, worked the tents, and kept it going!
Beautiful people doing AMAZING work to raise dollars and awareness for breast cancer!
A GORGEOUS 10 year survivor and her bestie volunteering and supporting all the walkers!Meet The Pink Crusader, who cheers us on and makes us smile at events! Way to Go!
The Incomparable Riley Weston, Actress, Singer, Writer, Author, Activist, and our TOP FUNDRAISER!!!!!
To all those in the thick of it with breast cancer, survivors, their caregivers and loved ones, and those who have lost loved ones too soon – we work for you!
Want to help? Here’s the Link to My Fundraiser! Or donate to your favorite survivor, team, or other nonprofit dedicated to eradicating breast cancer!
It’s day 14 of National Breast Cancer Awareness Month. Whew, a blog post a day is hard, y’all! But I hope these posts have been informative, entertaining, and full of hope. We all need hope. And we all need to be inspired.
That’s what I’m aiming for tomorrow. Between the pandemic and other turmoil in the world, it’s been over 4 years since I’ve done an in-person race/walk event. I still fundraised and still kept momentum going, but there is just something about seeing a sea of supporters – people with breast cancer, survivors, caregivers, loved ones, and everyone who shows up to raise money and shine a light on this awful disease!
There’s nothing quite like it.
I’ve seen beautiful bald women and women with gorgeous scarves, women with short and long hair spray painted pink, women who’ve traded illness for the graceful bodies of athletes, women with curves for DAYS rocking it, Black, Brown, White, Asian, Indigenous, gay and all the other letters of the alphabet mafia, old, young, and men who’ve also endured this horrible disease and stand in solidarity, not to be forgotten. It’s beautiful. It’s inspiring. It gives me the will to keep going!
Please, keep going!
I walk in memory of my cousin Sherri Killian, taken from us too soon by breast cancer, my uncle Jack, who we lost to cancer, and in honor of my mother, Carol Brantley, survivor. I walk in honor of my bestie Pam Jasper, and my friends Sue Daugherty Draughn, Linda Horton, Janet Piper, Karen Pugh, Tanisha Jones, and so many others who are more private about their cancer stories. So many family members, friends, colleagues, and acquaintances have been touched by cancer. We all know someone.
Sometimes we are that someone.
I walk for you. I may not know you personally, but we are connected. I work for you. I will not rest. If I can help one person, it is worth it. We fight cancer by holding one another up, celebrating victories, and witnessing and remembering those who leave us too soon. We fight.
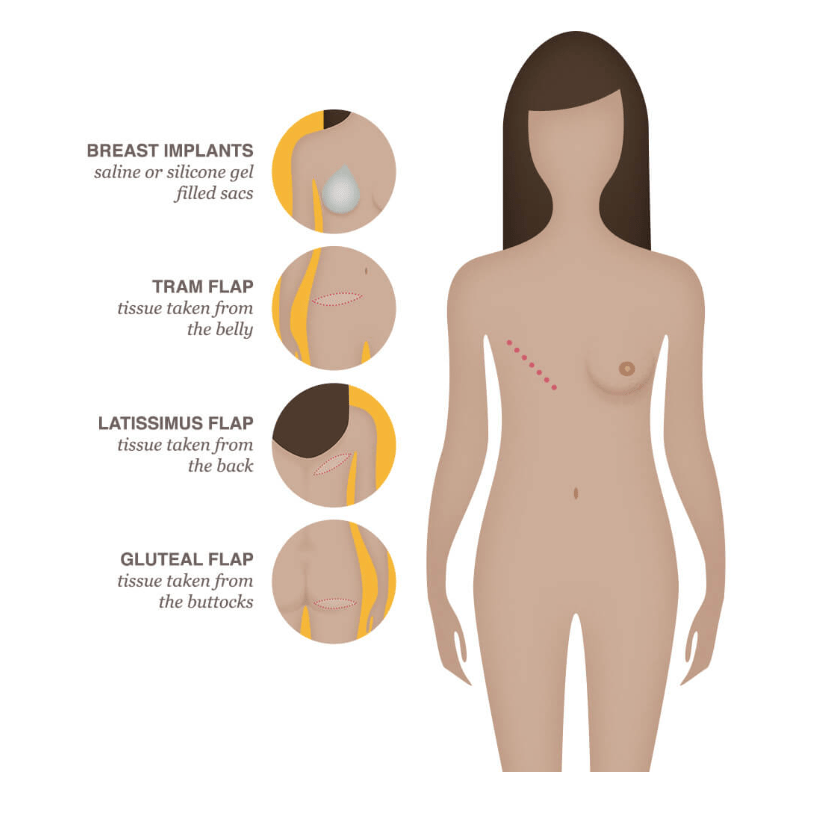
It’s day 13 of National Breast Cancer Awareness Month! Today, I’m taking a break from the usual programming to talk about my breast reconstruction journey, which I hope is (finally) over. I had the misconception that breast reconstruction was relatively simple, one or two procedures and done!
Image Source Here. Also has information about different types of reconstruction!
Yeah, that was before I got breast cancer. Oncoplastic reconstruction (lumpectomy followed by reduction and lift) was a one and done, as is (or can be) aesthetic flat closure (going flat). But building new breast(s) after mastectomy is complex and involves multiple surgeries/procedures to achieve symmetry and an aesthetically pleasing result. That’s where I’m at in the process.
I talk about this in Talking to My Tatas, and include pictures of where I was in the process as of 2021, but it might be useful to include a timeline and description of the various procedures I’ve had. Everyone’s reconstruction process is unique and tailored, but it should give you an idea of how involved the process can be and often is for people who’ve been diagnosed with breast cancer.
June 2018 – Tumor removal from left breast by lumpectomy and oncoplastic reconstruction
September 2018 – Radiation therapy on left breast
February 2020 – Diagnosed with residual disease in the left breast (at the beginning of the Covid-19 pandemic)
May 2020 – Unilateral mastectomy to remove left breast and to implant expander
(Involved several intervening procedures like 3X saline fills for expander and physical therapy to regain mobility after mastectomy, which was compounded by radiation damage to the skin over my left breast and breast tissue)
November 2020 – DUG flap reconstruction (grafting of thigh and muscle/skin tissue from right thigh to build foundation of left breast plus mastopexy (reduction and lift) on right breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
February 2021 – Liposuction and fat grafting into left breast + more tweaking on the right breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
July 2021 – Liposuction and fat grafting into left breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
December 2021 – Liposuction and fat grafting into left breast and scar revision on right breast
(Required lots of at home massage therapy on irradiated tissue to soften it)
October 2022 – Liposuction and fat grafting into left breast and minor scar revision on right breast
Image Source Here. Also has information on thigh flap reconstruction procedures.
That’s seven procedures, not counting biopsies and a lumpectomy from 2016 to remove a benign papilloma, in two years since residual disease detection. It’s a LOT! I count myself lucky to have a brilliant surgeon who has worked with me at my pace to get symmetry between a mostly natural right breast and reconstructed left breast, which is no easy task. And I have a great support system. But it’s a LOT. Each surgery involves recovery from anesthesia, incisions, bruises a plenty (lipo is brutal) and the mental and emotional impacts (which included depression and hypervigilance that made me feral). That required therapy, another part of the process.
Is it worth it? For me, the answer is yes. I’m almost back together and beyond amazed and pleased with how I look and feel. I am whole. Not the same, never the same, but whole. It’s a process. Remember that when you’re checking in with your survivor friends who may be waiting for follow-up procedures, tattoos or surgical nipple-building procedures, trimming of excess skin around incision areas, etc. It’s a process. Be kind. If you’re a survivor in the thick of reconstruction, remember to be kind to yourself and that YOU ARE WORTH IT!
While most breast cancers are sporadic, meaning there’s no genetic predisposition (i.e. gene variant inherited from one or both of your parents that increases your risk of breast cancer) that caused the cancer, around 5-10% of breast cancers are thought to be familial. Knowledge is power, and knowing if you have a genetic risk for breast cancer can empower you to take charge of your health by surveillance and managing your risk.
How do inherited gene variants increase a person’s risk for breast cancer? Everyone has two copies of genes that we inherit from our parents. These genes have many different variants in the human population, and some specific gene variants are associated with increased risk of breast cancer. For example, inherited mutations in BRCA genes that make the gene product non-functional (i.e. no longer able to repair damage to DNA) increase the risk for breast and other cancers because the loss-of-function allows other mutations to build up in affected cells, which can eventually transform them into cancer cells. If you carry BRCA variants associated with cancer, you may be at greater risk and you can also pass these risk genes to your children.
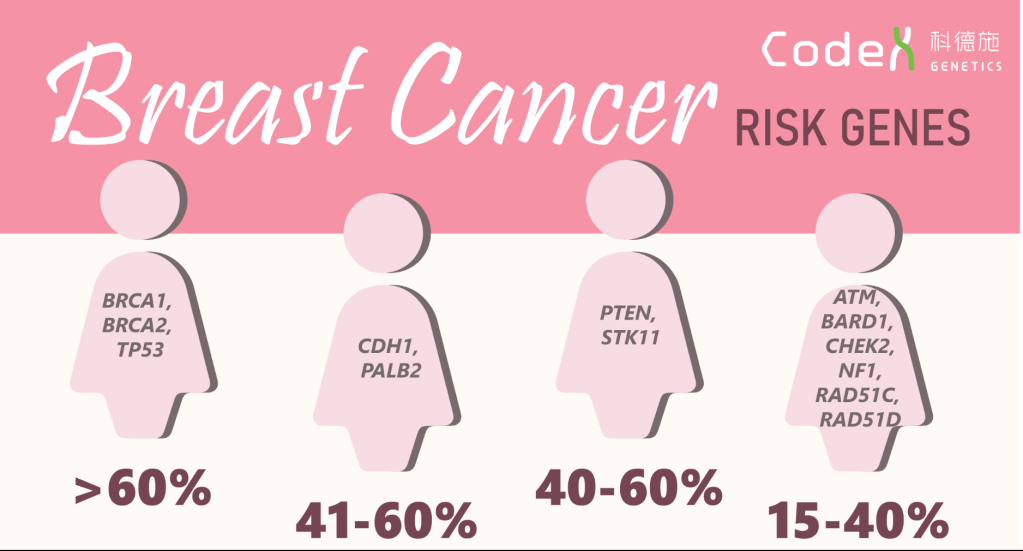
In addition to BRCA1 and 2 genes, other inherited gene variants have been identified that are associated with increased risk for breast cancer, as shown in the graphic below. Some of these genes, like TP53, PTEN, STK11, CHEK2, NF1, produce proteins that are also involved in regulating cell growth, so non-functional variants cannot put the breaks on cell growth and can cause cancer cells to grow uncontrollably. The PALB2, BARD1,ATM, and RAD51D gene products work like BRCA gene products to repair DNA damage, so loss of function increases the chance of accumulating mutations in cells, which can lead to cancer. The RAD51C gene product is involved in stopping cells with DNA damage from growing, so loss of function allows cells with mutations to divide and accumulate more mutations, which can lead to cancer.
Image Source Here. Percentages represent relative risk of breast cancer for people who have these gene variants associated with breast cancer.
Should you get genetic counseling and genetic testing? That’s a personal decision, but here are some recommendations from the CDC that might help you make your decision:
A strong family history of breast and ovarian cancer,
A moderate family health history of breast and ovarian cancer and are of Ashkenazi Jewish or Eastern European ancestry.
A personal history of breast cancer and meet certain criteria (related to age of diagnosis, type of cancer, presence of certain other cancers or cancer in both breasts, ancestry, and family health history).
A personal history of ovarian, fallopian tube, or primary peritoneal cancer.
A known BRCA1, BRCA2, or other inherited mutation in your family.
Knowing your risk can help you and your healthcare providers make decisions about surveillance and possible interventions. Take care of yourself, and if you can, find out about your family history of breast cancer.
It’s day 11 of National Breast Cancer Awareness Month! I’ve been so inspired, entertained (laughter is often the best medicine), and filled with pride by social media activity showcasing people working hard to raise breast cancer awareness, celebrating survivors, and sharing their stories!
Here are a few of my favorite videos for National Breast Cancer Awareness Month!
Indigenous Peoples Reminding Their Loved Ones to Book Their Mammograms!
This video featuring funny stories from deaf breast cancer survivors lit me up!
Funny stories from 4 deaf breast cancer survivors!
On of my favorite comedians, the incomparable Tig Notaro, tells us how to make breast cancer funny!
Tig is the BEST!
And last but not least, here’s a great story from another favorite comedian, the amazing Wanda Sykes!
It’s nice to not need a bra!
Got any favorites? Send me links! Sharing is caring, and we could all use a laugh!