Mike Judge.
In this installment of Screw The Woo Woo, I’m tackling a “wellness” trend that’s been making the rounds on social media, including my Facebook feed, and that is disturbing on sooooooooo many levels: butthole sunning. At first, I thought it was a joke. I really, REALLY hoped it was a joke. Then again, jade eggs for the vagina, vagina steaming, and coffee enemas were (and apparently still are) a thing, so what’s one more bizarre bit of ridiculousness in the wooniverse? This isn’t directly related to breast cancer, BUT(T), since ultraviolet light from the sun can cause skin cancer, I’ve decided to tackle the subject and debunk its alleged benefits to, er, bring to light the very real dangers of exposing your junk to the sun.
That and one of the proponents of this weird ass practice is making shady claims about how butthole sunning balances hormones in the sex organs. It doesn’t. More on that later.
First off, the notion that sunlight can enter your body through your vagina or anus is ludicrous, as is the notion that butthole sunning prevents the leakage of “chi” from the body, mostly because “chi” isn’t a thing, and if you’re experiencing any kind of leakage from your anus or genitals, you DEFINITELY need to seek your doctor. The vagina doesn’t just magically open to the heavens like a flower when you open your legs to the sun. Don’t believe me? Read The Vagina Bible by Dr. Jen Gunter, M.D. and gynecologist who covers everything you need to know about care and maintenance of your girly parts.
In addition to blocking chi leakage, woo woo practitioner MetaphysicalMegan (~a clearly qualified source of accurate, reliable information~) claims that sunning your perineum (a.k.a. the taint, the gooch, the fleshy fun bridge) provides a myriad of “health benefits“ (link to a story that shares her tweet – I refuse to link directly to woo woo bullshit sites) – such as regulating “hormone function in the sex organs.”
That claim is a GIANT steaming pile of bullshit.
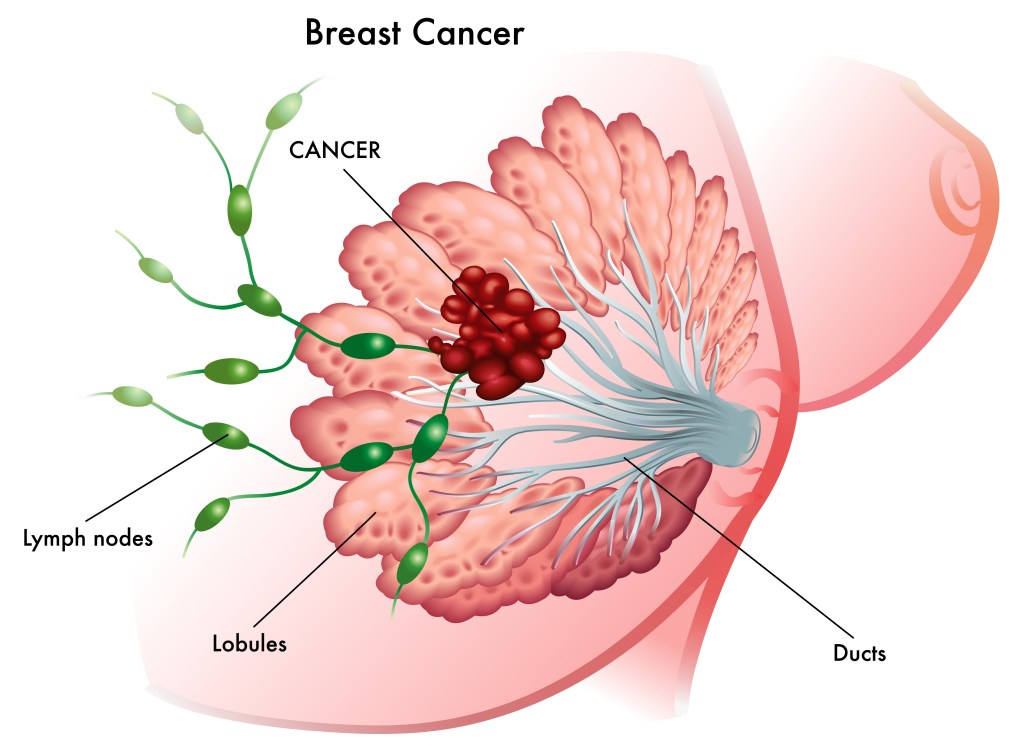
Hormone function in sex organs is regulated by intracellular hormone receptors expressed in the cells of internal sex organs that are well-protected from the outside world, including sunlight. For example, estrogen receptors in females are expressed in mammary glandular epithelium deep within breast tissue (where they can contribute to the growth of breast cancer cells in ER+ disease), the endometrial tissue that lines the uterus (internal organ protected from sunlight), ovary, bone (which is why bone loss is a concern for menopausal women and breast cancer patients on estrogen suppression therapy – estrogen contributes to cellular signaling pathways that promote bone growth), and other organs and tissues that are protected from the elements. As sunlight cannot reach estrogen receptor expressing cells, it cannot influence the function of estrogen signaling within them.
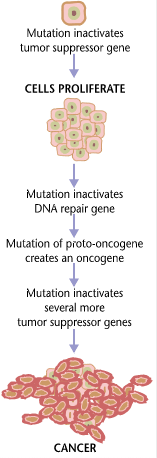
But what’s the harm, you might ask? Lots of people believe in and incorporate New Age and Wellness practices into their daily lives. Well, in this case, exposing delicate skin to ultraviolet sun rays without the benefit of sunscreen can actually be harmful. Ultraviolet light breaks bonds in the nucleotide bases (thymine and cyotsine) of DNA in skin cells that absorb it. This can facilitate abnormal bonding between adjacent thymine (thymine dimers) and cytosine (cytosine dimers) that form kinks in DNA. If not repaired, this can lead to DNA mutations that contribute to the development of skin cancers. Now, MetaphysicalMegan recommends 30 seconds, but given that every second you are in the sun, 50 to 100 of these dimers are formed in each skin cell. That’s a hell of a place to risk getting skin cancer, not to mention that the proverbial “places where the sun don’t shine” are horrible places to get a freakin’ sunburn!
Bottom (giggle snort) line: exposing your asshole/taint/vagina/penis/nutsack to the sun isn’t going to help your health. It’ll probably give you a sunburn, it can increase your risk of skin cancer, and it will most certainly make you look like a fucking idiot. Don’t do it.
Publicly available references from The US National Library of Medicine, National Institutes of Health: Estrogen receptor expression and function in female reproductive disease; Estrogen receptors and human disease: an update

*Apparently Josh Brolin tried butthole/perineum sunning and, not surprisingly, regretted it. Yup, not even Thanos can handle that flavor of sick burn. The evil part of me REALLY hopes that Ryan Reynolds works in some butthole sunning jokes at Cable’s expense in the next Deadpool film!
Maybe they’ll even do a little superhero bro bonding with joint butthole sunning. They could even bring along Colosus and Dopinder.
I mean, who DOESN’T want to see dat ass? You’re picturing it. I know you are!