One of the things I love about my work in advocacy is discovering amazing people who are doing the work and making a difference! Valeda Keys is one such remarkable person. She’s a Global Ambassador for Breast Cancer Awareness, using her platform and the Non-Profit organization she founded, Valeda’s Hope, to assist women in their journey from diagnosis to remission. She has one hell of a compelling story that includes a family history of breast cancer, a personal battle with breast cancer that included seven surgeries, and finding strength and empowerment in helping others.
When I learned about her work on LinkedIn, I was blown away.
Valeda, who is an Author, Speaker, LPN, Non-Profit Founder, Breast Health Navigator, and all around incredible human being, helped her mother through a breast cancer diagnosis, treatment, and later recurrence. A dream told her that she would one day endure her own battle with breast cancer, which unfortunately came true in 2010. Luckily, because of her family history, Valeda started receiving mammography screening at the age of 27 and kept up with her screenings, which allowed her healthcare team to detect her first breast cancer at an early stage. After a lumpectomy, she received the results of her genetic testing, which revealed that she carries a variant of theBRCA-2(BReast CAncer gene 2) gene associated with an increased risk of breast and ovarian cancer.
Everyone has two BRCA1 and two BRCA2 genes, but sometimes a variant of one of these genes that doesn’t work gets passed down from one of your parents. If something happens to the other copy of the BRCA gene in a cell (for example, a cell from your breast or ovary), it can increase your risk for cancer. Why? BRCA genes encode information to make proteins that help fix damage to DNA. DNA molecules encode and store all the information a cell needs to make proteins, which allows a cell to live and perform its function. When DNA is damaged, it messes with the code, and if the damage isn’t repaired, cells make defective proteins that don’t function well or in the case of cancer-causing oncogenes, function too well. Defects in some genes make cells grow uncontrollably, and sometimes those cells turn into cancer cells. Variants of BRCA genes that don’t function to fix DNA damage makes it more likely for oncogenes to get activated and make cells grow uncontrollably, leading to cancer. In the graphic above, you can see a DNA repair deficient breast cell in which the BRCA genes encode DNA repair proteins that don’t work. Because the defective BRCA gene produces a defective protein, the cell can’t repair DNA damage and gets a lot more mutations in a lot of different genes. Some of these mutations create defective proteins that let the cell grow uncontrollably, even without estrogen (E2) or other cues from the body that tell cells when to grow. See my Cancer 101 blog post and my other blog poston how cells become cancerous for a refresher on the cell biology of breast cancer, DNA damage and how it leads to cancer, and oncogenes.
End Science Break
Now, back to Valeda’s story. Since she carries a variant of BRCA-2 that doesn’t work, she was still at risk for getting another breast cancer or ovarian cancer after her first breast cancer diagnosis. She decided to keep her breasts and get screened more often, a valid choice. (Note: there are no right or wrong choices when it comes to keeping your breasts or having a double mastectomy. There are only informed choices you make with your healthcare team that are right for you.). She also endured radiation therapy that led to some serious complications, and was treated with tamoxifen, a drug that blocks estrogen function. In spite of this, she was diagnosed with a new breast cancer in 2011 and opted for a double mastectomy and autologous reconstruction (i.e. reconstruction using her own tissue from her abdomen to build new breasts), which unfortunately came with some complications, and later had a hysterectomy.
Through it all, she remained focused and determined not to let breast cancer get in the way of living a full life and achieving her goals. Her faith helped her through, and it gave her a mission to educate, empower, and help other women through their own breast cancer journeys. Among the many amazing things she does through Valeda’s Hope, Valeda sponsors a ton of mobile mammography events and encourages women to keep up with life-saving screenings. She shares her knowledge and experience through speaking engagements and educational events like Valeda’s Hope Pink & Pearls Luncheons. Valeda also hosts events that provide emotional and physical support as well as information about genetic testing for breast cancer risk genes, and so much more.
A fantastic book by an amazing survivor!
I’ve said it before, and I’ll say it again: the breast cancer survivor community is so supportive! Survivors support other survivors, patients, and caregivers. As a survivor, Valeda is using her voice and actions to help other women survive and thrive, and that deserves a spotlight, kudos, and celebration!
It’s funny. I’ve been meaning to write more blog posts, but I’ve been so busy with work, family, writing, and…COVID. My whole family got the ‘Rona and it sucked. Fortunately, we’d been vaccinated, and my husband and I had been boosted. It didn’t result in hospitalization or death. We were lucky. My birth mother, Mary Etta Caldwell, was not. We lost her to Covid and I’m still reeling. PSA – the pandemic isn’t over. It’s still killing people. It’s still debilitating people with long haul Covid. Get vaxxed/boosted and stay safe out there.
Now, onto the main event. This one’s a fucking RIOT!!!
I don’t know if this was from a bot, but I’d like to think it’s from a man. I picture a middle-aged white man who is possibly unemployed and likes to slide into women’s DMs and make sexist comments, spew pseudoscience woo woo, and is a fan of Trumplican propaganda on Facebook and Twitter. We’ll call him Arthur – because that’s what his profile says!
Arthur is very concerned about me and my health. So concerned, in fact, that he reached out in a very sincere and grammatically sound Facebook Message to save me. Now, he hasn’t read my book—though he promises he will and I totally believe him—but he has vital information that he must share with me. Aren’t I lucky?
Arthur has the secret to cancer. Are y’all ready? It’s a dry rot fungus addicted to sugar, and all you need to kill it is hot water.
Straight out of my Facebook Messenger!
But if I REALLY want to keep the fungus at bay, I need to “maintain a LOW GLYCEMIC diett” and since “your carryinga little extra weight,” I must still be eating a high glycemic carb “amoint.”
Now, I’ve received flak before for pointing out bad grammar and spelling in personal attacks, but come on! This fucker reached out to me, a breast cancer survivor and researcher, with unsolicited advice and, quite frankly, the STUPIDEST explanation for cancer I’ve ever heard—and I’ve heard some real doozies.
But, beyond the poor grammar, spelling, and general stupidity, there is so much more fodder here for me to unpack. Firstly, mansplaining. It’s a thing. Ask any woman in your sphere and she’ll tell you. She won’t even have to think about it, and will probably come up with five personal experiences in less than a minute. I am an expert in the field of breast cancer. Not sort of, kind of, I guess I know a little—I’m a bona fide expert in the field with a Ph.D. and more than twenty years of experience studying the disease. I also have personally experienced breast cancer IN MY BODY. I know what I’m talking about, and the information I share is carefully researched and derived from peer-reviewed scientific publications.
And yet, like so many mediocre white male living examples of Dunning-Kruger, he just couldn’t help himself! Yes, I’m singling out white men. No, I don’t think it’s out of line. If you’re a white man and you’re offended, then you’re an Arthur and you need to rethink your life choices and behavior. If you’re not offended, you’re an ally and you should call out the Arthurs in your life because they’ll listen to you as a fellow white man. You can do it. It’s easy and fun.
Next, the fungus thing. I don’t think Arthur is giving white rot fungus a fair shake. Apparently, it is quite a useful organism that plays a vital role in the global carbon cycle by breaking down lignin, an organic polymer component of plant cell walls, especially in wood and bark, that lends rigidity and do not rot easily. If we didn’t have dry rot fungi, we’d have a whole lot of dead trees mucking up the planet.
But Dr. Dana, does it cause cancer??
Of course not!* In fact, an early pre-clinical study performed in colon cancer cell lines reported that extracts from a species of dry rot fungus, Cerrena unicolor, caused cancer cells to die in culture. That’s right, my friends. I think white rot fungi should sue Arthur for slander. Arthur is spreading malicious propaganda against this very useful organism that does more good on planet earth than Arthur could ever hope to achieve. Clearly, Arthur is jealous.
Now, as for sugar and cancer, it’s complicated. Biology is complicated. Anyone who says anything different is trying to sells you bullshit supplements. I wonder if Arthur sells supplements… Anyway, metabolism consists of a complex series of interconnected biochemical reactions that convert food energy into cellular energy required to fuel cellular processes, generate building blocks necessary to create/sustain/repair biomass, and eliminate cellular waste. Metabolism gets fucked up in very interesting ways in cancer cells and in the cells that surround it (microenvironment). Obesity is a metabolic health issue and a risk factor for breast cancer.
However, as noted by the American Cancer Society, “But the connection between weight and breast cancer risk is complicated. Studies suggest the risk appears to be increased for women who gained weight as an adult but may not be increased among those who have been overweight since childhood. Also, having extra fat in the waist area may raise risk more than having extra fat in the hips and thighs.” There are many, many dedicated, highly trained, competent scientists and physicians studying the complexities of metabolism, and there’s plenty they still don’t know.
I guarantee they know WAAAAAAAAAAAAY more about the subject than Arthur, who has no medical degree, no credentials, and no peer-reviewed studies to back up his assertions. The only thing he has is the audacity. As for the not-so-subtle dig on my weight, I can’t say it better than Lizzo. I’m a big bitch. I don’t have a tour bus, but I’ve got a degree, a platform, and I do a lot of good in the world. What do you do that’s worth anyone’s while, Arthur?
Lizzo is the undisputed QUEEN and I ADORE HER!
*If you want to hate on fungi linked to cancer, you should really go for Aspergillus flavus and Aspergillus parasiticus. They produce aflatoxins, and exposure to those increases liver cancer risk.
In summary, in a world full of Arthurs, be a Lizzo.
I was going to end it here, but Arthur slid back into my DMs to leave these little nuggets of wisdom:
From my Facebook Messenger – It’s an interesting place.
No, I’m not clicking on any of those links, because I don’t want a computer virus. Somehow, I don’t think this is the only virus Arthur is carrying. I hope you’ve found this post informative and entertaining, because I had a HOOT writing it! Thank you, Arthur.
The book has been out for about 3 weeks and I’ve been thrilled/nervous/pee-my-pants-excited to see my Amazon ranking as well as checking for ratings and reviews on Amazon, Goodreads, and other retail sites like Barnes & Noble, Walmart, Google Books, and Rowman & Littlefield!
For a brief, beautiful, shining moment, it was the #1 New Release in Breast Cancer and Oncology on Amazon, and I have the screenshots to commemorate it!
Pics or it didn’t happen!
Want a sneak peek? Of course you do! Here’s an excerpt from Chapter 16 that deals with an exciting new development in cancer research and treatment – harnessing the patient’s own immune system to seek out and destroy cancer cells through immune checkpoint inhibitors.
EXCERPT
I’ll also take comfort in the fact that we’re getting new weapons in the arsenal for fighting breast cancer. Antitumor immunity is the hottest thing to hit the field of cancer research since the 2001 approval of Gleevec (a game-changer drug used to treat chronic myelogenous leukemia that targets the oncoprotein product of the Philadelphia chromosome that drives the disease) and the 2006 approval of Gardasil (first vaccine targeting the human papilloma virus strains that cause most cervical cancers). Recently Frontiers in Immunology published the history of antitumor immunity efforts leading to the development of immune-checkpoint inhibitors available in the clinic today, the use of engineered T-cells taken from patients and altered to fight their cancer, and oncolytic viruses.2 I’ll go over the basics, including how antitumor immunity works and the challenges we still face in getting tumors to respond.
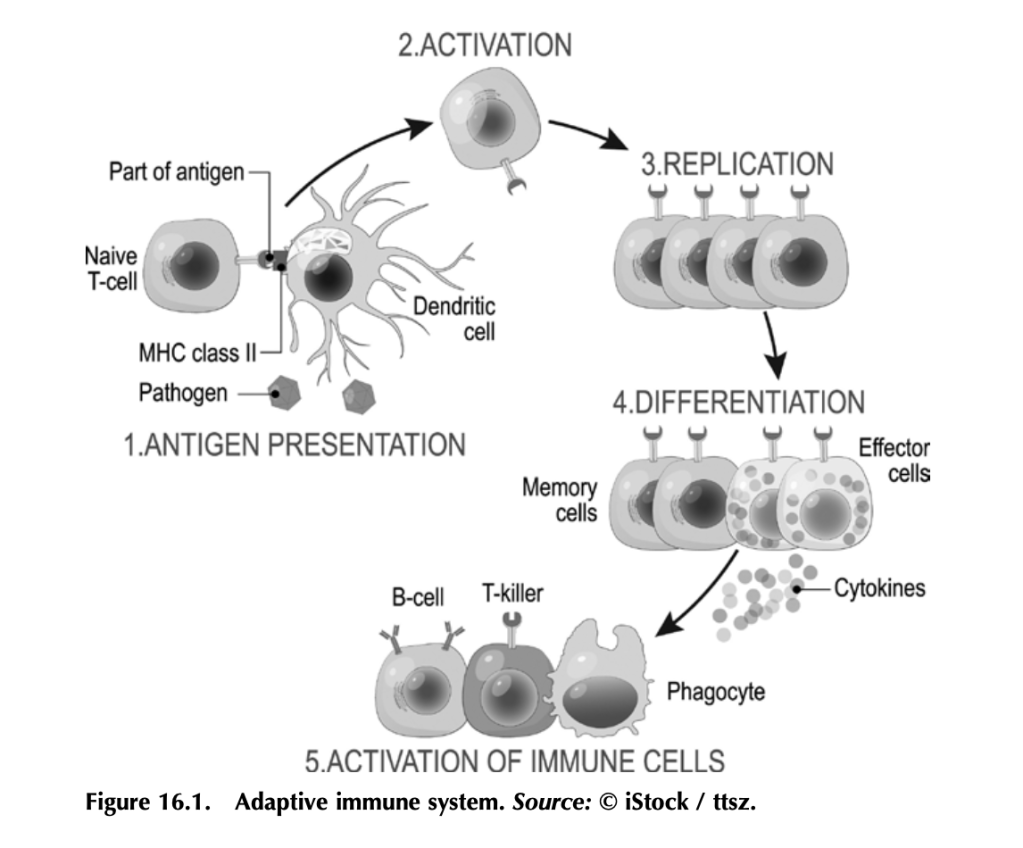
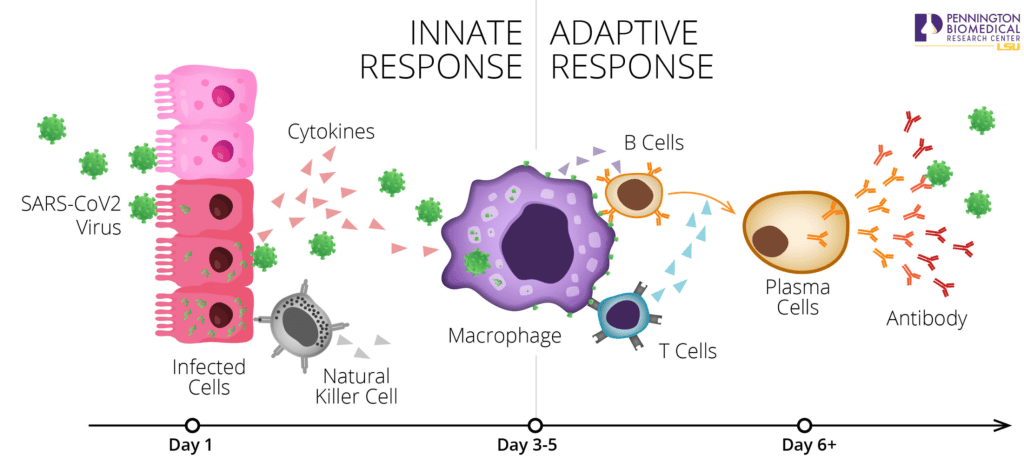
Before we get into how antitumor immunity works, we need to understand how the immune system works to fight infection. It’s a complex beast, but here are some basics. Your immune system functions to mount a rapid and robust defense when your body encounters a pathogen (e.g., a virus or bacteria that causes disease) in your daily life. The arm of the immune system that does this is called the adaptive immune system (figure 16.1). The other arm is the innate immune system, which includes natural barriers like skin, the tiny hairs and mucous in your nose, and stomach acid. The adaptive immune system is what antitumor immunity treatments harness. It is also altered by tumors to suppress tumor immune responses and exploited to work for the tumor. (More on that in a bit.)
The adaptive immune system works like this: Specialized cells identify a potential threat (e.g., an infection), and they carry information about that threat in the form of bits of protein called antigens to other immune cells. If the threat is credible, those immune cells get activated and fight the threat. First the specialized cells that identify a potential threat patrol your body, looking for something suspicious. Cells like macrophages and dendritic cells, which roam around various organs and tissues, find pathogens (a bacteria, virus, or other microbe that causes disease) or unhealthy cells infected by pathogens, and eat them (the fancy term is phagocytosis). Infected or damaged cells send out protein signals called cytokines as a distress call to attract these patrolling macrophages and dendritic cells. While “digesting” the bacteria or infected cell, macrophages and dendritic cells salvage proteins or pieces of proteins—antigens—that identify the bacteria or virus as “other,” and they present these to immune cells, usually in lymph nodes, which in turn mount an immune response. Macrophages and dendritic cells are known as professional antigen presenting cells (APCs).
When activated by APCs, immune cells called B-cells produce antibodies against the antigen, which can do a lot of things to fight an infection. Some antibodies neutralize the pathogen by binding it and stopping it from entering a cell. Other antibodies tag infected cells as a signal for other immune cells to come and kill them. Others coat pathogens or infected cells in a process called opsonization (meaning “the process of making tasty”), which signals other cells like macrophages to come and eat the coated pathogens or cells. Specialized B-cells called memory B-cells store the information about the antigen so your immune system can recognize the pathogen when it hits you again and mount a faster immune response.
Other immune cells called T-cells, which are particularly relevant to antitumor immunity, become activated by APCs and mount a different kind of immune response. Cytotoxic T-cells seek out and kill infected or damaged cells, and helper T-cells help activate B-cells so they make antibodies, activate cytotoxic T-cells, and activate macrophages to go eat nasty invaders and infected cells. Memory T-cells also store information about past infections to mount a rapid, strong response the next time your body sees it.
That’s a simplified but hopefully digestible explanation of immunity and the major players (there are other immune cells, but APCs, B-cells, and T-cells are the biggies).
Memory is key to protection, and memory is built by exposure to pathogens.
Put a pin in that concept for when we get to anticancer vaccines, and also remember what T-cells do for when we get to engineered CAR T-cells and oncolytic viruses.
Working out how to harness your body’s own immune system to fight cancer isn’t a new idea. It’s been under investigation since the nineteenth century. In fact, in chapter 5 we covered the way trastuzumab (trade name Herceptin), a humanized anti-HER2 antibody, targets HER2-expressing breast cancer cells for death. Herceptin and other monoclonal antibodies mimic the natural activity of antibody- producing B-cells to deliver therapies and tag cancer antigen–expressing cells for immune-mediated destruction. But it was the discovery of checkpoint inhibitors—proteins that put T-cells in a state of exhaustion and inactivity in pathways that are exploited by many cancers— that led to the first molecularly targeted therapies designed to boost antitumor immunity. Doctors James Allison and Tasuku Honjo pioneered this Nobel Prize–winning work.3
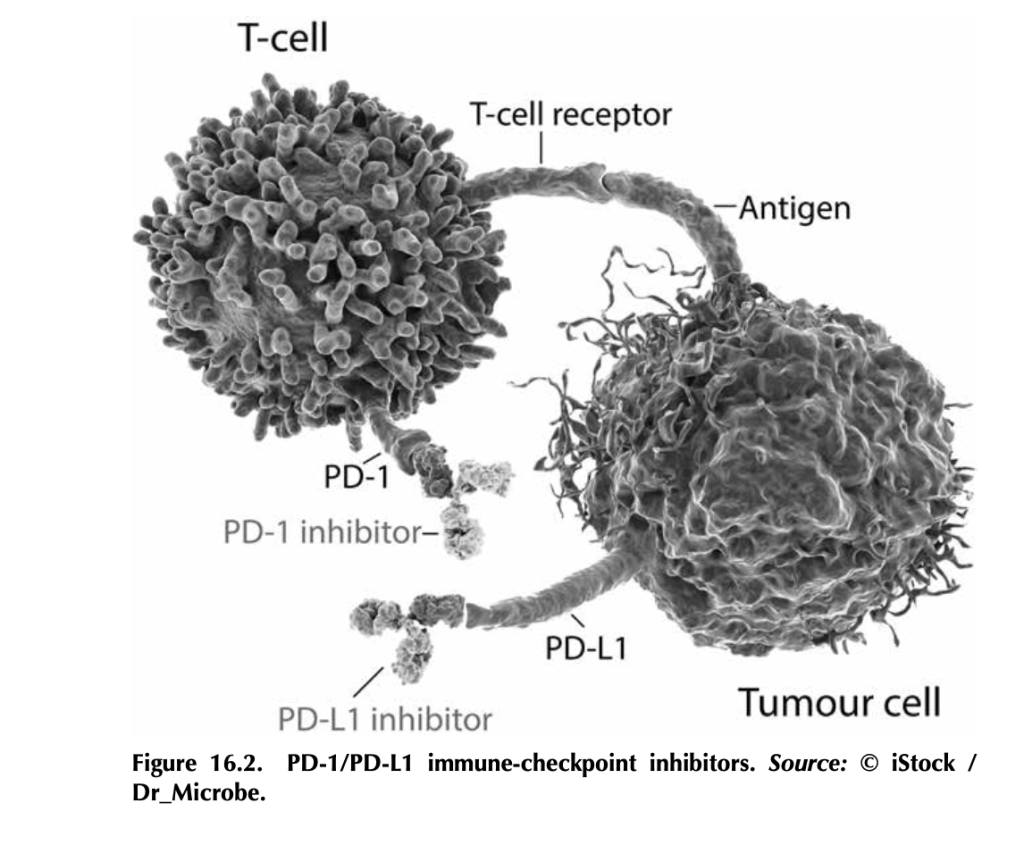
What are immune-checkpoint inhibitors, and how do they work? T- cells, particularly cytotoxic T-cells that actively kill their targets, bind to antigens on tumor cells through their T-cell receptors. But tumor cells, being the adaptable beasts that they are, can produce proteins like PD-L1 (programmed death ligand 1), which bind to PD-1 (programmed cell death protein 1), proteins on T-cells. This interaction tells the T- cell to stand down by tricking it into thinking that the tumor cell is “self” and should be protected. Signaling networks like this normally promote self-tolerance so that your immune system doesn’t attack your own healthy cells (figure 16.2). In tumors, it works by telling tumor- infiltrating T-cells, if present, to go into a state of inactivity. Drugs that target PD-L1—like atezolizumab (trade name Tecentriq), durvalumab (trade name Imfinzi), and avelumab (trade name Bavencio)—and drugs that target PD-1—like nivolumab (trade name Opdivo) and pembrozolimuab (trade name Keytruda)—are FDA-approved mono- clonal-antibody therapies that block interactions between PD-1/PD-L1 to unleash an antitumor immune response.4
Other immune-checkpoint molecules exploited by cancers include cytotoxic T lymphocyte antigen 4 (CTLA-4), the target of the first FDA-approved immune-checkpoint inhibitor ipilimumab (trade name Yervoy). Approved in 2011 for advanced melanoma, this drug had remarkable results. In fact, over 20 percent of the patients enrolled in the initial ipilimumab clinical trials (before the 2011 approval) are still alive and show no evidence of disease (NED).
There’s some incredible potential in targeting checkpoint inhibitors.
CTLA-4 is part of a cellular-signaling pathway that normally fine- tunes immune responses. CTLA-4 and a similar receptor, CD28, are expressed on two different T-cell types: (1) CD4+ helper T-cells, which help activate other immune cells to mediate adaptive immune responses, and (2) CD8+ cytotoxic T-cells, those cells that kill infected cells, damaged cells, and, if properly activated, tumor cells. Antigen- presenting cells make a protein called B7, which can bind to either CD28 or CTLA-4 on T-cells, and the effects on T-cell function are very different depending on what B7 binds. If it binds to CD28, B7 activates T-cell responses as a part of a complex of proteins that includes the T-cell receptor. Binding of B7 to CTLA-4 shuts down T- cell functions. CTLA-4 probably serves as protection from self-antigen recognition by inducing immune suppression, since laboratory mouse models engineered to not express CTLA-4 die from autoimmunity. This is the aspect of CTLA-4 function that gets highjacked by tumor cells. Drugs like ipilimumab block the suppressive activity of CTLA-4, which can allow T-cells to attack tumor cells.5
Here’s the kicker: The tumor actually has to have infiltrating T-cells for this to work, and not all tumors do. Tumors with T-cells that can be activated to fight the tumor are called “hot,” whereas tumors without T-cells are “cold.” One of the most aggressively researched topics in tumor immunology right now is how to make a cold tumor hot and thus responsive to antitumor immune therapies.
This is especially important for breast cancer, since most subtypes produce cold tumors. Right now, immune-checkpoint therapies are only approved for advanced triple-negative breast cancers that make the PD-L1 protein. Not all triple-negative breast cancers make PD-L1. Ongoing research is looking to expand the use of immune therapy in inflammatory breast cancer and the HER2+ subtype.6 Hopefully, with more research, we’ll figure out how to make more tumors responsive to immune therapy by making them hot (full of T-cells) and by discover- ing other immune checkpoints that can be targeted.
3. Heidi Ledford, Holly Else, and Matthew Warren, “Cancer Immunologists Scoop Medicine Nobel Prize,” Nature, October 1, 2018, https://www.nature. com/articles/d41586-018-06751-0.
4. See American Cancer Society medical and editorial content team, “Immunotherapy for Breast Cancer,” Treating Breast Cancer, American Cancer Society, Cancer.org, last revised December 3, 2020, https://www.cancer.org/ cancer/breast-cancer/treatment/immunotherapy.html.
6. Devon Carter, “Does Immunotherapy Treat Breast Cancer?” MD Anderson Center (website), University of Texas, March 26, 2021, https://www .mdanderson.org/cancerwise/does-immunotherapy-treat-breast-cancer.h00 -159385101.html.
I can’t believe I have to write this post. I’m shaking my head and weeping for the future of humanity as I write it. Are people really stupid enough to believe that ivermectin – a drug we use in our laboratory mice to treat pinworms (butt worms) – can cure Covid?
Yes (sadly). Yes, they are.
This is what came up when I searched for Ivermectin. I have to adjust the search…These are related searches…people, just, just don’t…
Ivermectin is used to treat butt worms in animals. It can also be used to treat roundworms in people. It works by paralyzing worms, specifically by binding to proteins on motor neurons (nerves that tell muscles to move) and disrupting their activity. It also mucks around with the ability of nematode worms to reproduce.
Fun fact: the naturally occurring analogs of ivermectin, avermectins, were discovered in bacteria from soil samples collected by Dr. Satoshi Ōmura from woods near a golf course in Kawana, on the south east coast of Honshu, Japan. The name “avermectin” reflects the activity of these compounds, making treated organisms “worm free.” Dr. Ōmura and Dr. William Campbell shared the 2015 Nobel Prize in Physiology or Medicine for this discovery. You can read more about that here. Ivermectin in pill form can be used in humans to treat parasitic worms, and topical (on the skin) formulations are also used to treat head lice and rosacea.
It does actually have other, non-butt worm related activities that include treatment of severe muscle spasticity in patients with spinal cord injuries and shows activity against leukemia in laboratory animal models. It may also target molecular pathways relevant to treatment of other cancers, including lung and colon cancer and glioma based on laboratory animal studies, and could block inflammatory T-cell activity in atopic dermatitis, relieving irritation. A recent review covers the research on these applications.
Okay, given these other potential applications, I guess I can kinda sorta see why some folks without a science background might be buying into the idea of using Ivermectin to treat Covid, but(t) still…
This apparently became trendy because of ongoing clinical trials designed to test the efficacy of Ivermectin for Covid-19 treatment and prevention, alone and in combination with other drugs.
Why? Because laboratory studies (in petri dishes in a lab, NOT in people) have shown that Ivermectin can inhibit viral replication, which means it can stop the virus from making copies of itself, which is how it spreads. In vitro. In vitro means “performed or taking place in a test tube, culture dish, or elsewhere outside a living organism.” Plenty of other previous studies showed that ivermectin blocks replication or interferes with the production and spread of other viruses, including HIV, Dengue virus, West Nile virus, and a few others. In vitro. You can review some of these studies here. In spite of these in vitro studies, there is no evidence that ivermectin has any anti-viral effect on the SARS-CoV-2 virus that causes Covid-19. For a link to clinical trial data, click here.
And misuse of ivermectin can be dangerous. According to theFDA,“Even the levels of ivermectin for approved human uses can interact with other medications, like blood-thinners. You can also overdose on ivermectin, which can cause nausea, vomiting, diarrhea, hypotension (low blood pressure), allergic reactions (itching and hives), dizziness, ataxia (problems with balance), seizures, coma and even death.”
The best way to limit the spread of SARS-CoV-2 is to get the vaccine. Period.
And Now for the PSA I never thought I’d have to make…
About the whole so-called “urine therapy” thing – something I never in a million years imagined I would blog about. It isn’t a thing. Apparently, some anti-vaxx conspiracy theory wingnut named Christopher Key has been encouraging his followers to drink their own urine to ward off the SARS-CoV-2 virus instead of getting vaccinated.
Kids, please don’t take advice from people with mugshots…
For the sake of being thorough and due diligence, I performed a PubMedsearch for “urine therapy covid” on January 16. The search produced 188 results, most dealing with the effects COVID-19 on kidney function, studies related to the potential spread of the virus through urine (risk reported to be negligible), urine-based COVID-19 testing and analysis of cytokines and other diagnostic markers, and testing for SARS-CoV-2 in waste water.
The funniest result was a paper with the title, “Influence of perceived threat of Covid-19 and HEXACO personality traits on toilet paper stockpiling” published inPLoS One.
This one was more sad than funny, but apparently some folks in India are using cow dung to treat COVID-19. People…rubbing animal shit and urine all over your body isn’t effective at treating ANYTHING and is likely to expose you to a whole lot of nasty zoonotic (spread by animals) diseases. Plus you’ll stink. Just…don’t.
You know what I didn’t find in my literature search? I didn’t find a single peer-reviewed study endorsing the use of drinking your own piss as a treatment for COVID-19. Zero, zip, zilch, nada – no evidence to back up this ridiculous claim.
Not that the crazies need silly things like evidence. This actually fits quite nicely with the all-natural woo woo trends. Can you picture it? All natural, locally sourced, sustainably harvested on tap pee pee for your health needs! You’ve heard of eating placenta (don’t do that, either), but why stop there? Drink your pee! When it’s fresh, it looks like a beer.
Sure doesn’t taste like beer. Stick to drinking nice, cold brewskies, and get your vaccine. Please.
It’s been a while. This is my first post for Breast Cancer Awareness Month 2021, but I promise I’ve been busy in the laboratory. In the past two months, I’ve submitted grant applications to Breast Cancer Alliance, METAvivor, and Department of Defense CDMRP Breast Cancer Research Program. The first two are foundations that fund novel research projects, supporting scientists like me so we can take a chance on new projects that are higher risk/high reward and generate preliminary data for larger funding proposals. DOD supports larger research projects at both early (Breakthrough Level 1) and later (Breakthrough Level 2) stages. Fingers and toes crossed for grant funding! If you’re looking for organizations to support, I highly recommend Breast Cancer Alliance and METAvivor.
For this post, I’d like to highlight some survivor communities that have helped me and continue to help me, and to encourage patients and survivors to reach out for support. Cancer made me feel powerless. Sure, I was taking care of myself and following instructions from my surgeons, oncologist, and other providers, but they were doing things to me and for me – cutting out the cancer, managing my followup therapies, monitoring me to make sure the cancer wasn’t back, but I felt like I wasn’t (or couldn’t) do anything. That’s part of the reason I wrote Talking To My Tatas and why I started this blog. I needed to DO something.
I also needed to know I wasn’t alone. Enter other breast cancer patients and survivors. These people are some of the most generous human beings, providing support, practical advice, sharing their stories, and giving lots and lots of love to people who join this club we never wanted to be a part of but is filled with survivors in every sense of the word.
Where can you find support? Plenty of places! The Internet can be a terrible and wonderful place, and in the case of support for cancer patients and survivors, it can be a lifeline. Here are some survivor communities who’ve helped see me through on Facebook:
This is a large FB group dedicated to shared experiences and full of practical advice! I went to them when I was preparing for my mastectomy and I got a TON of tips for what to expect, what to stock up on (soft cotton camis and cardigans with pockets for surgical drains, pillows, etc.). Need advice from folks who’ve been there? Need to vent? Looking for hope? A safe place to express yourself? This is a great one!
Laughter is one of the best weapons we have when it comes to cancer, and you’ll get plenty of laughs from this group. Lots of boob humor. Check them out!
Want to know about the latest research? Looking to connect with survivors and get involved in advocacy, or do you need information on resources from financial to physical and mental health? This group is a great place to start.
Looking for a support community that welcomes patients and survivors outside of majority faith communities? This one is super helpful and supportive!
Not big on social media? Ask about support groups available through your medical center. Check out your local Gilda’s Club – just be sure to follow safety guidelines for Covid-19. Need a support community for African American breast cancer patients and survivors? Check out Sisters Network – they provide a space for African American breast cancer patients to meet, bond, and receive support during treatments. Similar organizations tailored to the unique needs and experiences of other communities of color include: The Latino Cancer Institute, The American Indian Cancer Foundation, and The Asian American Cancer Support Network. Support for LGBTQIA+ cancer patients, including a directory for LGBT-friendly cancer treatment facilities, can be found at The National LGBT Cancer Network.
No matter your background, culture, or identity, you don’t have to go it alone when it comes to breast cancer. I encourage you to find your support network and lean on them. And, when you’re ready, be a part of that community and give your support to someone in need.
A cancer diagnosis affects all aspects of a person’s life, and that includes employment. Coupled with the astronomical cost of cancer healthcare, especially for the un- and underinsured, the short and long term impact of cancer on financial stability and employment can be disastrous. If you are female, a person of color, disabled, and/or LGBTQIA+, these negative impacts are very often compounded by sexism, racism, ableism, and homophobia.
Sexism, racism, discrimination, and other biases make working, maintaining productivity, and feeling valued for your work much more challenging in the face of cancer. I’ll cover some of those challenges in this post, as well as protections in place within the United States to alleviate them (with the caveat that we need more), and additional policies and protections that we could implement to protect and support cancer patients and survivors in the workplace. I’ll focus on breast cancer, but many of these challenges and solutions apply to people diagnosed with other types of cancer.
What are some of the challenges cancer patients and survivors face when it comes to work and careers? According to a recent study published in the Journal of Clinical Oncologychallenges like job loss, decreased earnings, and increased spending (the last two described as “financial toxicity”) are some of the greatest. It seems like a no-brainer: if you lose your job or part of your income plus healthcare coverage while the medical bills for treatments pile up, you’re not really surviving all that well financially, let alone thriving. But we like and trust peer-reviewed data here, so let’s look at data.
Financial distress caused by job loss/lost wages not only makes you feel worse, it has also been linked to “increased symptom burden and emotional distress and to decreased quality of life and treatment adherence.” In other words, if you’re strapped for cash or you’re suffering from the mental health effects of a cancer diagnosis without resources, you’re not as likely to be treatment or medication compliant. That leads to poor outcomes. Worse, cancer patients are more than twice as likely to file for bankruptcy after diagnosis, and bankruptcy is associated with almost double the risk of death among survivors.
That’s the biggie, and adds insult to injury. You have to pay for your treatments in order to live, but you may have to go bankrupt to do it, which increases your risk of DYING!
2. The scope is significant. Around 45% of people diagnosed with cancer in the United States are working age (20-64). This affects a LOT of people, y’all!
3. Many, if not most, people diagnosed with cancer do not have the means, privilege, or opportunity to take leave, paid or unpaid, for treatments, even under the Family and Medical Leave Act (FMLA). In fact, only 21% of low wage workers have access to paid sick leave. And for many workers who do, there aren’t protections in place to make certain they can return to their jobs following treatment. The Americans with Disabilities Act (ADA) provides protections for cancer patients against workplace discrimination and requires employers to make reasonable accommodations to allow cancer patients to continue to work, but it only applies to employers who have 15 or more workers. And a significant percentage of low wage workers are employed by small businesses that are exempt from FMLA and ADA requirements.
These are the same essential workers we’ve failed as a nation to support during the global pandemic.
4. Aside from concrete challenges, the mental and emotional health costs of a cancer diagnosis can reduce social engagement and a patient’s sense of self worth. I work as a cancer researcher and a cancer center, have a TON of privilege, and even I’m not immune to these challenges*. If I’m not, imagine how awful it is for patients and survivors with fewer resources and protections.
5. I cover disparities related to cancer care, outcomes, and financial toxicity in my book, but suffice to say, if you are female, not white, not able bodied, and not straight, you are likely to disproportionately experience all of these challenges on a much more significant level thanks to racism, sexism, homophobia, and ableism.
Existing and Future Solutions
In addition to FMLA and ADA protections (for those who qualify), many non-profit organizations offer financial assistance to cancer patients. Funds are available from Susan G. Komen for the Cure, the American Cancer Society, Young Survival Coalition, and other organizations, many of which I cover in my book, that can be used to cover the costs of treatments, bill pay, home health care and childcare, and a variety of other expenses.
But to truly and comprehensively tackle this issue, we need systemic changes. Some of the more so-called “progressive” solutions, like universal healthcare coverage, tend to be met with skepticism or outright hostility from free-market (*cough, cough – rich, white conservatives – cough, cough*) advocates who complain about lack of “personal responsibility,” think the current system works just fine, and/or think vouchers for purchase of private insurance and other non-government solutions work better (even though universal healthcare works very well in most other industrialized nations).
Aside from universal healthcare, there are other initiatives that have worked in other nations that might appeal to conservatives while making a significant impact on job retention and financial stability for cancer patients and survivors. For example, as noted in the Journal of Clinical Oncology Society study cited above, “A 2012 systematic review evaluated the effectiveness of government policies in place from 1990 to 2008 in Canada, Denmark, Norway, Sweden, and the United Kingdom to change employer behavior with regard to return to work. The most successful policies included financial incentives for employers to hire people with disabilities; flexibility and adaptations in the work environment, particularly with flexible schedules and giving employees more control over work demands; and programs that involved employers in return-to-work planning.” These incentives benefit everyone, including employers, patients/survivors, and society as a whole.
Patient-oriented interventions that tackle physical, psycho-educational, and/or vocational portions of cancer patients’ employment retention were associated with higher return-to-work rates compared to patients who received standard care. And patients who received this type of multidisciplinary intervention “experienced a significant increase in perceived importance of work, work ability, and self-efficacy with regard to returning to work, and return to work was 59%, 86%, and 83% at 6, 12, and 18 months, respectively.”
It’s going to take a lot of work in the form of political will, advocacy, legislation, and incentives to solve this problem. What can you do to help? Contact your elected officials and voice your support for programs that support cancer patient financial stability and access to reliable and affordable healthcare, job retention, and return to work with appropriate accommodations. It’s the right thing to do, and it’s good for the economy, society, and humanity.
If you’ve experienced workplace discrimination based on your status as a cancer patient/survivor, click here for information about your rights and what you can do to protect them.
*Story Time
You’d think being a cancer researcher who works at an academic institution dedicated to cancer care, research, and saving and improving the lives of those diagnosed with cancer, I’d be immune to the bullshit discussed above.
In many ways, I am. Thanks to a supportive Department Chair and Division Chief (both female), I was granted an extension on my tenure clock, additional discretionary funds, and professional/personal support from my (largely female) colleagues. To these individuals, I see you. I appreciate you. I love you.
Then there are the (largely male) colleagues who have made my experience working while undergoing cancer treatment and returning to work after the Covid-19 shutdown and a (very short) medical leave a lot shittier. My passion for breast cancer researcher didn’t diminish when I was diagnosed. I became MORE passionate! I worked through radiation treatments, horrible systemic therapies while trying to find one I could live with for 10 years, and after surgeries when I remained swollen, sore, fatigued, and mentally struggling with all of the emotional fallout associated with cancer.
And yet…a peer reviewer for a grant I submitted felt the need to make the following comment in his (I’m 99.999999% certain it’s a dude) review summary: “Dr. Brantley-Sieders is an Assistant Professor of Medicine…who completed her Postdoctoral fellowship in 2003. A concern is her lack of productivity, with only a single first or last author publication since 2017, and only 4 in total since 2012. That said, as noted in her letter of support by [DEPARTMENT CHAIR], she is a breast cancer survivor and there may be circumstances that underlie her less than optimal extent of productivity.”
First of all, it’s not true. I had and have more first/senior author publications since 2017 and 2012. In fact, I have published over 55 papers in high tier journals, which demonstrates my highly collaborative approach to science. Secondly, WHAT THE ACTUAL FUCK??? This reviewer thought it was okay to weaponize my own breast cancer diagnosis on a grant I submitted to a BREAST CANCER RESEARCH ORGANIZATION in the presence of other BREAST CANCER SURVIVORS serving as consumer reviewers. But, since my application wasn’t de-identified, and with my hyphenated last name (for which I’ve received inappropriate feedback about), this reviewer felt entitled to pose this outrageous and untrue criticism on an application by a female scientist.
Rather than hiding in a corner to lick my wounds, I reported this to the organization starting with leadership. Was it a risk? Of course! Backlash and retaliation are always a risk, especially for women who dare to speak out. But, if I stayed silent, I would have become part of the problem. I refuse to do that. I’ll be part of the solution.
I’m in the middle of another situation with a colleague I once trusted (my mistake) that centers around perceived shortcomings related to how I am balancing my work and ongoing treatments. What started as a communication issue is rapidly escalating into something more serious. At best, it’s a problematic situation. At worst, it may represent a serious violation of policy. I hope to resolve it in a way that is fair and satisfactory to both parties, but the damage is done in terms of trust and my perceived value to the project. Again, I could just sit quietly and accept it, but I’m not going to be part of the problem. I’m a fighter. I’m a damned good researcher who has made and will continue to make valuable contributions to science, and I’m worth it.
Talking to My Tatas: A Breast Cancer Researcher’s Adventure With The Disease And What You Can Learn From It is scheduled to be published February 8, 2022!
On. My. 49th. Birthday.
I’m not one for signs, but this is the second serendipitous date associated with this book baby so far. The first was getting the offer for publication from Rowman & Littlefield on November 5 of last year, the same day I was in surgery for the first step in my left breast reconstruction. This is the second. I am filled with joy and delight!
What’s next in the process? Now that I’ve turned in finalized chapters and other components of the book with edits in response to super helpful comments and notes from editor Suzanne Staszak-Silva (shout out to my amazing literary agent Barbara Collins-Rosenberg for giving me edits and notes prior to sending them to Suzanne), the manuscript enters the production phase. I’ll be receiving notes from the Production Editor, completing any revisions, going through proofs, reaching out for endorsements – shout out to the folks who already said, “Yes, send it to me for an endorsement!” – and planning for the release and promotion.
I cannot WAIT to see the cover!
I also cannot wait until this book is available to the public, including the hundreds of thousands of newly diagnosed breast cancer patients, current patients, survivors, and caregivers. If I can help even one of those people – my survivor sisters and brothers – by informing them, inspiring them, helping them cope, or giving them a much needed laugh, then I will have accomplished something really special.
This book will also help me develop a guide for newly diagnosed breast cancer patients at my institution, another labor of love.
I send love and gratitude to all of the mentors and colleagues who’ve made me into the scientist I am today, my healthcare team for saving my life and helping me thrive, and my family for being my strength and limitless supply of love.
Facebook is a great place to meet some weird-ass motherfuckers. We all know that. But I’m still surprised and more than a little dismayed by the scammers. I normally just report ads that include woo woo, sometimes leaving a snarky comment, or just hide or block scammers. It’s rare that they actively seek me out, but it does happen.
Check this out! In response to my post on a blog post about legitimate, peer-reviewed science and breast cancer, Mr. Ansari was compelled by the power of the spell caster, “Dr” Akhigbe, to testify about the amazing things the spell caster can do.
It’s an impressive list worthy of the most outrageous scammy chiropractor. He apparently has the cure for herpes (HSV – I assume the genital variety), HIV, gonorrhea, low sperm count, menopause disease (it’s not a disease, even if it feels like it sometimes; he’s big on STDs and fertility), epilepsy, asepsis (I think he means sepsis – “asepsis” refers to aseptic techniques that minimize risks of bacterial, fungal or viral contamination during surgery and medical procedures), and cancer (which kind, dude?).
Where has this paragon of the medical community been all my life? Why haven’t we heard of him?
I have a few theories, but I decided to go down the rabbit hole and read more about the good “doc” and his miraculous healing abilities. First off, he has at least three profiles. Sketchy. The spell caster profile is apparently now dedicated to marriage, fertility, and “total freedom and happiness.” Hmm, I wonder how much that costs?
The posts are a feast of stock photos with tons of woo, attractive people who seem to be happy, and hashtags a plenty (candlemagic #magicspells #candlespells #astrology #occult #spellcandles #witchyvibes #bruja #pagan #witches #astrologer #psychicreading #witchcraftspells #spellcraft #conjurer #metaphysical #lovespecialist #spellcasters #brujasofinstagram #spiritualoils #spellworker #moneyspells #spiritualawakening #healing #lovespellsmaster #follow #spellcandlesofinstagram #spiritual #altarsofinstagram).
Yup. He’s a busy, busy man. There’s a lot going on there…
I kind of hope there’s a mockumentary based on this dude. Not that it would be as good as What We Do In The Shadows, but I’d LOVE Colin Robinson to explain the history of herbal medicine to The Spell Caster until he’s utterly drained.
I’ll focus on the other profile, which deals with herbal remedies for “great diseases,” because “it’s a gift from God.”
Here’s one of his posts related to cancer:
I’ve already covered turmeric, antioxidants (this includes the berry thing), and I’m covering mushrooms in my book, so let’s dig into what garlic and ginger can do for you (and more importantly, cannot do for you) as a cancer patient.
Note: My medical oncologist is a fan of veggies as well as legitimate research on diet and breast cancer molecular signaling/drug responses. Check out his blog for legit information and some great recipes!
Garlic. It makes food delicious, your breath stinky, and wards off vampires, but what can it do for cancer? When I searched the web, the first promising result I found was from Memorial Sloan Kettering Cancer Center. Reputable enough for me! When I clicked, a big fat pop up window with a disclaimer and a “Continue” button I had to click to proceed tried to jump out of the screen:
“This Web site — Information About Herbs, Botanicals and Other Products — is for general health information only. This Web site is not to be used as a substitute for medical advice, diagnosis or treatment of any health condition or problem. Users of this Web site should not rely on information provided on this Web site for their own health problems. Any questions regarding your own health should be addressed to your own physician or other healthcare provider.”
They have a whole disclaimer to protect them from yahoos looking for woo woo!
What did it have to say about garlic? In terms of cancer, here’s the 411:
Getting into the nuts and bolts, the clinical summary (with references) states:
1. Possible correlation with garlic supplement and gastric (stomach) cancer mortality (death) but not incidence (getting cancer), but other studies found no evidence of either. Remember, correlation does NOT equal causality.
2. Mixed results on garlic and colorectal cancer, with some observation of reduced number and size of adenomas (precancerous lesions) in patients with a history of adenomas.
3. Mixed or unclear results on risk of other cancers, but possible association with reduced risk of blood cancer. Remember, correlation does NOT equal causality.
Bottom line: garlic makes food tasty! Enjoy it in your favorite recipes, but don’t rely on it to keep you safe from cancer or to treat your cancer.
As far as ginger, I found a great article that already covers it:
“Walk Gingerly Before Declaring Ginger a Cancer Cure It is not at all unusual to find plant extracts that will kill cancer cells in vitro. There are hundreds of phytochemicals that will do this. Neither is it unusual to find an effect in mice that have implanted tumours. But this is a long way away from demonstrating a viable cancer treatment in humans.”
Bottom line: this pretty much sums up the majority of studies on plant extracts and cancer. Enjoy ginger for the flavor, but don’t count on it to cure your cancer.
With the recent emergency use approval of two independent vaccines for SARS2-CoV-2, the virus responsible for the horror that is Covid-19, many folks have questions: What the heck are these vaccines? Are they safe and effective? Should I get one?
Note: I’m not going to dignify any wild conspiracy theories about vaccines and microchips. Bill Gates doesn’t care about you or me or anyone else he doesn’t know and he has better things to do that track you with a microchip in a vaccine. Seriously. People believe some weird shit… If anyone wanted to track you, they’d do it digitally by your freakin’ cell phone.
That being said, the first three questions are completely legit. My goal in this post is to break down the science behind the Pfizer and Moderna vaccines, what we know so far about their safety and effectiveness, and dispel some common misconceptions about them.
First, here’s a crash course on how your immune system fights infections. This is important, since vaccines harness the power of your immune system to mount a rapid and robust defense if and when you encounter the actual pathogen (i.e. virus or bacteria that cause disease) in your daily life. The arm of the immune system that does this is called the adaptive immune system. The other arm is the innate immune system and includes natural barriers like skin, the tiny hairs and mucous in your nose, and stomach acid.
How does the adaptive immune system work? First, it involves cells that roam around your body looking for something suspicious. Cells like macrophages and dendritic cells, which patrol various organs and tissues, find pathogens like bacteria or unhealthy cells infected by viruses like SARS-CoV-2, and eat them (fancy word is phagocytosis). Infected or damaged cells send out protein signals called cytokines as a distress call to attract macrophages and dendritic cells. While “digesting” the bacteria/infected cell, they salvage proteins or pieces of proteins—antigens—that identify the bacteria or virus as “other,” and they present these to immune cells, usually in lymph nodes, that mount an immune response. Macrophages and dendritic cells are known as professional antigen presenting cells (APCs)
When activated by APCs, immune cells called B-cells produce antibodies against the antigen, which can do a lot of things to fight an infection. Some antibodies neutralize the pathogen by binding it and stopping it from entering a cell. Other tag infected cells for other immune cells to come and kill them. Others coat pathogens or infected cells in a process called opsonization (meaning to “make tasty”), which signals other cells like macrophages to come and eat the coated pathogens/cells. Specialized B-cells called memory B-cells archive the information about the antigen so your immune system can recognize the pathogen when it hits you again and mount a faster immune response.
Other immune cells called T-cells become activated by APCs and mount a different kind of immune response. Cytotoxic T-cells seek out and kill infected or damaged cells, and helper T-cells help activate B-cells so they make antibodies, activate cytotoxic T-cells, and activate macrophages to go eat nasty invaders and infected cells. Memory T-cells also archive information about past infections to mount a rapid, strong response the next time your body sees it.
That’s a simplified by hopefully digestible explanation of immunity and the major players (there are other immune cells, but APCs, B-cells, and T-cells are the biggies). Memory is key to protection, and memory is built by exposure to pathogens.
But what if there was a way to expose your body to pathogens without making you sick? That’s where vaccines come in!
The way vaccines work is to tap into this process and activate the adaptive immune response using an artificial antigen supplied by the vaccine, getting your immune response geared up and, importantly, building those archival memory B- and T-cells that will recognize the real infection when your body encounters it so it can rapidly fight it. Types of vaccines include: Live-attenuated vaccines; Inactivated vaccines; Subunit, recombinant, polysaccharide, and conjugate vaccines; Toxoid vaccines.
Live-attenuated means using a weakened form of the virus to initiate an immune response—examples include measles, mumps, and rubella (MMR) and chickenpox vaccines. Inactivated means using a dead version of the virus that cannot infect cells but contains antigens that can be used to activate adaptive immunity—examples include flu, hepatitis A, and rabies vaccines. Subunit, recombinant, polysaccharide, and conjugate vaccines use pieces of the virus that act as antigens, like proteins and sugars—examples include HPV, hepatitis B, and shingles vaccines. Toxoid vaccines use toxins produced by the pathogen to mount an immune response against the toxic protein—examples include tetanus and diphtheria vaccines.
What the heck are these (Covid-19) vaccines?
The current FDA approved (for emergency use) Covid vaccines from Pfizer and Moderna belong to a newer class called mRNA vaccines. See my previous post on DNA to mRNA to protein (Central Dogma of Molecular Biology) for a refresher on mRNA. This is really just a modification of the subunit, recombinant, polysaccharide conjugate vaccine approach in that it delivers messenger RNA coding for the SARS-CoV-2 spike protein, which the virus uses to enter a cell, instead of delivering the spike protein itself. See my previous post on SARS-CoV-2 for information about the spike protein. The cells in your body that take up the mRNA make spike proteins themselves, which in turn activates your immune system and provides protection.
Are they safe and effective?
Since these are new vaccines approved for emergency use, and since due to the accelerated nature of their development and approval, some people are understandably wary of their safety and ability to protect against Covid.
While they may be new, a lot of the groundwork for these vaccines started in in 2002 with the emergence of the first SARS virus (SARS-CoV) and continued with study of the related MERS-CoV virus. SARS-CoV uses the same spike protein to enter target cells through angiotensin-converting enzyme 2 (ACE2). Scientists learned a great deal about coronaviruses by studying SARS-CoV and MERS-CoV, including how to develop vaccines.
Let’s look at safety first. Clinical trials involving tens of thousands of healthy volunteers have been performed. Safety concerns include allergic reactions to the vaccine or components of the vaccine. Providers who deliver the vaccine are equipped to deal with anaphylaxis on site, which is why you’ll be asked to hang around for 15 minutes after your shot just in case. You might feel feverish, fatigued, and generally yucky the day after one or both shots (the first activates the immune system and the second gives it a signal boost), which is NOT a sign that you have Covid. It actually means your immune system is working, building memory and its arsenal of weapons to fight Covid if you encounter the real virus.
The FDA is continuing to monitor those who received the vaccines in clinical trials, as well as those who received the vaccines after emergency approval. So far, they appear to be safe.
As far as effectiveness, data from trials looking at the number of Covid-19 cases in trial participants relative to the total number of participants revealed that the Pfizer vaccine is 52% effective after the first shot (39 cases of covid-19 in the vaccine group and 82 cases in the placebo group) and 95% effective after the second shot (8 covid-19 cases in the vaccine group and 162 cases in the placebo group; 43,448 trial participants) – New England Journal of Medicine (NEJM). Similar efficacy was reported for the Moderna Vaccine in NEJM.
There’s still a lot we don’t know – most importantly, we don’t know how long immunity produced by these vaccines will last. Some experts hypothesize they might provide a year or two of immunity, after which you’ll need more shots, but we won’t know until we see in real time as we track vaccinated people.
Should you get the vaccine?
Me getting my first dose of the Pfizer vaccine!
The more people who are vaccinated against this virus, the better. Vaccines will slow the spread of the virus by preventing infections in vaccinated people. Along with mask wearing and social distancing, the vaccines are a vital tool in stopping this pandemic. As a cancer survivor, I’m in a high risk category, meaning Covid-19 could kill or debilitate me. The same is true for people with diabetes and other underlying medical conditions.
That’s why I got my vaccine! Had the second shot a few days ago, which gives me peace of mind as I prepare to return to work after reconstruction surgery. I’m with Dr. Fauci on this one, and I encourage everyone to talk to their healthcare providers about getting vaccinated.
First off, HUGE news! My amazing literary agent, Barbara Collins Rosenberg, landed a publishing deal for me with Rowman & Littlefield!!! I’m honored, thrilled, and still squee-ing! So, stay tuned for Talking to My Tatas: A Breast Cancer Researcher’s Adventure With The Disease And What You Can Learn From It.
Here’s the Working Blurb – it will likely change based on guidance from my amazing editor, Suzanne Staszak-Silva, but it will give you a taste of what I intend to share (my story) and spread (scientifically sound information) with this book:
Can I talk to you about my personal relationship with my breasts?
I’ve spent twenty years working as a biomedical breast cancer researcher. Then, I was diagnosed with breast cancer. I thought I knew breast cancer before it whacked me upside my left boob and left me bleeding on the curb of uncertainty. Turns out, I had a lot to learn. The purpose of this book is to share my personal adventure with breast cancer, from the laboratory bench to my own bedside, and to provide accessible information about breast cancer biology for non-scientists. I say adventure, because I’d rather think of it as an action movie with some really cool side quests instead of another tragedy-to-triumph saga. I’m not big on sagas. I am big on kickass intellectual badassery, pathological nerdiness, and talking about my sweet, sweet rack.
Why do we need another cancer memoir? In a sea of inspirational stories, celebrity survivor stories, and physician memoirs that bring a clinical perspective, nothing I’ve found in the current market tackles breast cancer through the lens of a breast cancer researcher who became a survivor. We live in an age of fake news and pseudoscience, made worse by the pervasive anti-intellectual and anti-science political culture gripping the United States and much of the world. The Internet and social media are plagued by scammers selling “alternative medicine” and woo woo “cures” for cancer. Through Talking to My Tatas: A Breast Cancer Researcher’s Adventure With Breast Cancer And What You Can Learn From It, I offer accurate, evidence-based science that is accessible to laypersons, including the more than three hundred thousand individuals diagnosed with breast cancer every year*, their caregivers, and their loved ones.
Knowledge is power, and lack of it can lead to overtreatment, unnecessary pain and suffering, and can even be deadly. By demystifying the process from mammograms, biopsies, pathology and diagnostics, surgical options, tumor genomic testing, and new treatment options, I aim to offer hope in a story intended to blend the humor and delivery style of Jenny Lawson’sLet’s Pretend This Never Happened (A Mostly True Memoir) with the integrity and scientifically sound beauty of Siddhartha Mukherjee’s The Emperor of All Maladies: A Biography of Cancer.
*American Cancer Society Facts & Figures 2020
I’ve got some work to do! In addition to writing and fleshing out chapters for my editor to review (and work her magic on), I’ve been busy working on figures and visuals for the book, cover art forms, marketing and promo plans, and getting a new headshot! The one I currently have on this page and all over the Internet is absolutely gorgeous, fun, and from 2012. A LOT has happened in 8 years, and I have aged. I’d like to think I’ve aged gracefully, but at any rate, it was time to update the image.
Lillian Boeskool is MAGIC! She made me look so good and captured the essence of my personality in a series of amazing headshots (If you’re in the greater Nashville area and need headshots or other photography, HIRE HER). I have two favorite images and I cannot decide which one to use for this page and the book. I invite y’all to enable my decision-making disorder vote for your favorite!
Photo Credit Lillian B Photography
This one on the left is super fun and catches me trying not to laugh at something funny Lillian said and/or did. It captures my mischief, my sense of humor, and really makes my face look nice.
And, unlike the previous headshot for which I straightened my hair, this one highlights my popping natural curls!
I’m almost 48 years old. Anything that makes my face look nice is gold.
Told you she was MAGIC!
Photo Credit Lillian B Photography
There’s just something about this next one on the right that speaks to me.
I think it captures my sass and tells my readers that I’m going to take them on a really funny adventure that will make them a smidge uncomfortable but will ultimately leave them laughing and glad they went along for the ride.
That’s me in a nutshell.
I can’t decide between the two!
And…just to throw a monkey wrench into this whole program…
Photo Credit Lillian B Photography
This one is my husband’s favorite.
It’s nice, too.
I’m glad he thinks I look good in all of these photographs and still thinks I’m beautiful in spite of time marching across my face and body and in spite of cancer leaving me with a janky left breast-in-progress*.
He’s pretty awesome!
I think I’ll keep him.
*Janky left breast-in-progress on display in the first two photos as the line of discoloration just above my shirt collar. Lillian asked if I wanted to Photoshop it out, but I said no. It’s where I am right now. It’s why I’m blogging, writing this book, and becoming a breast cancer patient/survivor advocate as well as a breast cancer researcher. It’s a badge of fucking honor and it stays!