Use the promo code 22JOYSALE at checkout to get the sale price now through January 6, 2023!
This is a great deal, as you’ll save over $12 on the Hardback and almost $12 on the eBook. Know someone who is going through breast cancer? This would be a helpful gift. Know someone who’s a science loving nerd? They’ll probably like it, too!
It’s day 26 of National Breast Cancer Awareness month! Today, I had the opportunity to appear on the Tampa Reads segment of Fox 13 in Tampa with anchor Linda Hurtado! I was able to share my breast cancer story with a bit about science, about my personal story, and a bit about Talking to My Tatas.
It was a great experience and I hope I convinced some viewers to schedule their mammograms! Shout out to Linda Hurtado, Lisa Emerson, and the rest of Fox 13 News Team!
The book has been out for about 3 weeks and I’ve been thrilled/nervous/pee-my-pants-excited to see my Amazon ranking as well as checking for ratings and reviews on Amazon, Goodreads, and other retail sites like Barnes & Noble, Walmart, Google Books, and Rowman & Littlefield!
For a brief, beautiful, shining moment, it was the #1 New Release in Breast Cancer and Oncology on Amazon, and I have the screenshots to commemorate it!
Pics or it didn’t happen!
Want a sneak peek? Of course you do! Here’s an excerpt from Chapter 16 that deals with an exciting new development in cancer research and treatment – harnessing the patient’s own immune system to seek out and destroy cancer cells through immune checkpoint inhibitors.
EXCERPT
I’ll also take comfort in the fact that we’re getting new weapons in the arsenal for fighting breast cancer. Antitumor immunity is the hottest thing to hit the field of cancer research since the 2001 approval of Gleevec (a game-changer drug used to treat chronic myelogenous leukemia that targets the oncoprotein product of the Philadelphia chromosome that drives the disease) and the 2006 approval of Gardasil (first vaccine targeting the human papilloma virus strains that cause most cervical cancers). Recently Frontiers in Immunology published the history of antitumor immunity efforts leading to the development of immune-checkpoint inhibitors available in the clinic today, the use of engineered T-cells taken from patients and altered to fight their cancer, and oncolytic viruses.2 I’ll go over the basics, including how antitumor immunity works and the challenges we still face in getting tumors to respond.
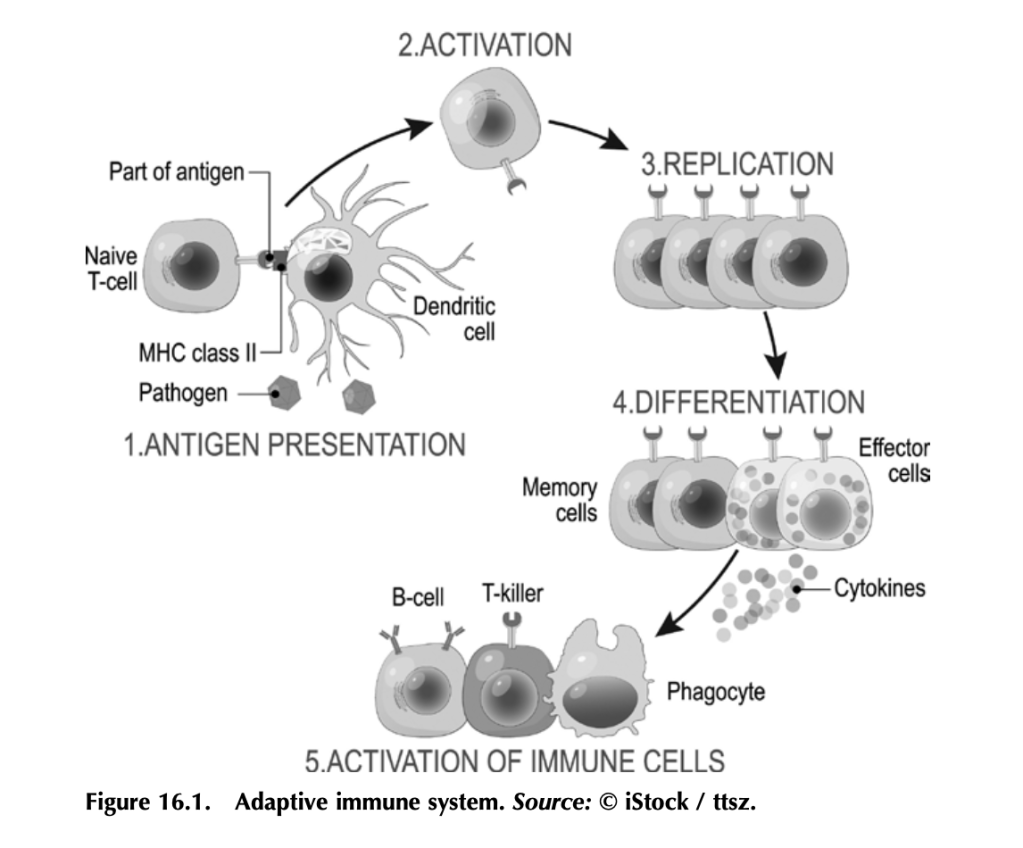
Before we get into how antitumor immunity works, we need to understand how the immune system works to fight infection. It’s a complex beast, but here are some basics. Your immune system functions to mount a rapid and robust defense when your body encounters a pathogen (e.g., a virus or bacteria that causes disease) in your daily life. The arm of the immune system that does this is called the adaptive immune system (figure 16.1). The other arm is the innate immune system, which includes natural barriers like skin, the tiny hairs and mucous in your nose, and stomach acid. The adaptive immune system is what antitumor immunity treatments harness. It is also altered by tumors to suppress tumor immune responses and exploited to work for the tumor. (More on that in a bit.)
The adaptive immune system works like this: Specialized cells identify a potential threat (e.g., an infection), and they carry information about that threat in the form of bits of protein called antigens to other immune cells. If the threat is credible, those immune cells get activated and fight the threat. First the specialized cells that identify a potential threat patrol your body, looking for something suspicious. Cells like macrophages and dendritic cells, which roam around various organs and tissues, find pathogens (a bacteria, virus, or other microbe that causes disease) or unhealthy cells infected by pathogens, and eat them (the fancy term is phagocytosis). Infected or damaged cells send out protein signals called cytokines as a distress call to attract these patrolling macrophages and dendritic cells. While “digesting” the bacteria or infected cell, macrophages and dendritic cells salvage proteins or pieces of proteins—antigens—that identify the bacteria or virus as “other,” and they present these to immune cells, usually in lymph nodes, which in turn mount an immune response. Macrophages and dendritic cells are known as professional antigen presenting cells (APCs).
When activated by APCs, immune cells called B-cells produce antibodies against the antigen, which can do a lot of things to fight an infection. Some antibodies neutralize the pathogen by binding it and stopping it from entering a cell. Other antibodies tag infected cells as a signal for other immune cells to come and kill them. Others coat pathogens or infected cells in a process called opsonization (meaning “the process of making tasty”), which signals other cells like macrophages to come and eat the coated pathogens or cells. Specialized B-cells called memory B-cells store the information about the antigen so your immune system can recognize the pathogen when it hits you again and mount a faster immune response.
Other immune cells called T-cells, which are particularly relevant to antitumor immunity, become activated by APCs and mount a different kind of immune response. Cytotoxic T-cells seek out and kill infected or damaged cells, and helper T-cells help activate B-cells so they make antibodies, activate cytotoxic T-cells, and activate macrophages to go eat nasty invaders and infected cells. Memory T-cells also store information about past infections to mount a rapid, strong response the next time your body sees it.
That’s a simplified but hopefully digestible explanation of immunity and the major players (there are other immune cells, but APCs, B-cells, and T-cells are the biggies).
Memory is key to protection, and memory is built by exposure to pathogens.
Put a pin in that concept for when we get to anticancer vaccines, and also remember what T-cells do for when we get to engineered CAR T-cells and oncolytic viruses.
Working out how to harness your body’s own immune system to fight cancer isn’t a new idea. It’s been under investigation since the nineteenth century. In fact, in chapter 5 we covered the way trastuzumab (trade name Herceptin), a humanized anti-HER2 antibody, targets HER2-expressing breast cancer cells for death. Herceptin and other monoclonal antibodies mimic the natural activity of antibody- producing B-cells to deliver therapies and tag cancer antigen–expressing cells for immune-mediated destruction. But it was the discovery of checkpoint inhibitors—proteins that put T-cells in a state of exhaustion and inactivity in pathways that are exploited by many cancers— that led to the first molecularly targeted therapies designed to boost antitumor immunity. Doctors James Allison and Tasuku Honjo pioneered this Nobel Prize–winning work.3
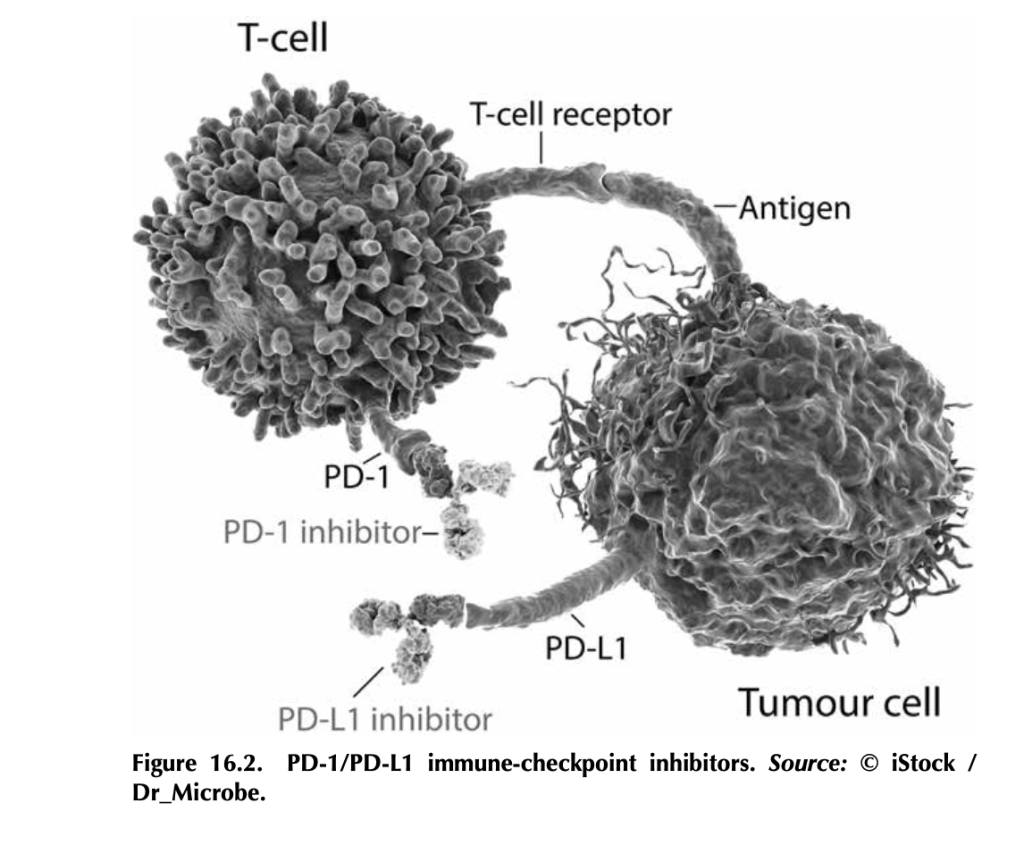
What are immune-checkpoint inhibitors, and how do they work? T- cells, particularly cytotoxic T-cells that actively kill their targets, bind to antigens on tumor cells through their T-cell receptors. But tumor cells, being the adaptable beasts that they are, can produce proteins like PD-L1 (programmed death ligand 1), which bind to PD-1 (programmed cell death protein 1), proteins on T-cells. This interaction tells the T- cell to stand down by tricking it into thinking that the tumor cell is “self” and should be protected. Signaling networks like this normally promote self-tolerance so that your immune system doesn’t attack your own healthy cells (figure 16.2). In tumors, it works by telling tumor- infiltrating T-cells, if present, to go into a state of inactivity. Drugs that target PD-L1—like atezolizumab (trade name Tecentriq), durvalumab (trade name Imfinzi), and avelumab (trade name Bavencio)—and drugs that target PD-1—like nivolumab (trade name Opdivo) and pembrozolimuab (trade name Keytruda)—are FDA-approved mono- clonal-antibody therapies that block interactions between PD-1/PD-L1 to unleash an antitumor immune response.4
Other immune-checkpoint molecules exploited by cancers include cytotoxic T lymphocyte antigen 4 (CTLA-4), the target of the first FDA-approved immune-checkpoint inhibitor ipilimumab (trade name Yervoy). Approved in 2011 for advanced melanoma, this drug had remarkable results. In fact, over 20 percent of the patients enrolled in the initial ipilimumab clinical trials (before the 2011 approval) are still alive and show no evidence of disease (NED).
There’s some incredible potential in targeting checkpoint inhibitors.
CTLA-4 is part of a cellular-signaling pathway that normally fine- tunes immune responses. CTLA-4 and a similar receptor, CD28, are expressed on two different T-cell types: (1) CD4+ helper T-cells, which help activate other immune cells to mediate adaptive immune responses, and (2) CD8+ cytotoxic T-cells, those cells that kill infected cells, damaged cells, and, if properly activated, tumor cells. Antigen- presenting cells make a protein called B7, which can bind to either CD28 or CTLA-4 on T-cells, and the effects on T-cell function are very different depending on what B7 binds. If it binds to CD28, B7 activates T-cell responses as a part of a complex of proteins that includes the T-cell receptor. Binding of B7 to CTLA-4 shuts down T- cell functions. CTLA-4 probably serves as protection from self-antigen recognition by inducing immune suppression, since laboratory mouse models engineered to not express CTLA-4 die from autoimmunity. This is the aspect of CTLA-4 function that gets highjacked by tumor cells. Drugs like ipilimumab block the suppressive activity of CTLA-4, which can allow T-cells to attack tumor cells.5
Here’s the kicker: The tumor actually has to have infiltrating T-cells for this to work, and not all tumors do. Tumors with T-cells that can be activated to fight the tumor are called “hot,” whereas tumors without T-cells are “cold.” One of the most aggressively researched topics in tumor immunology right now is how to make a cold tumor hot and thus responsive to antitumor immune therapies.
This is especially important for breast cancer, since most subtypes produce cold tumors. Right now, immune-checkpoint therapies are only approved for advanced triple-negative breast cancers that make the PD-L1 protein. Not all triple-negative breast cancers make PD-L1. Ongoing research is looking to expand the use of immune therapy in inflammatory breast cancer and the HER2+ subtype.6 Hopefully, with more research, we’ll figure out how to make more tumors responsive to immune therapy by making them hot (full of T-cells) and by discover- ing other immune checkpoints that can be targeted.
3. Heidi Ledford, Holly Else, and Matthew Warren, “Cancer Immunologists Scoop Medicine Nobel Prize,” Nature, October 1, 2018, https://www.nature. com/articles/d41586-018-06751-0.
4. See American Cancer Society medical and editorial content team, “Immunotherapy for Breast Cancer,” Treating Breast Cancer, American Cancer Society, Cancer.org, last revised December 3, 2020, https://www.cancer.org/ cancer/breast-cancer/treatment/immunotherapy.html.
6. Devon Carter, “Does Immunotherapy Treat Breast Cancer?” MD Anderson Center (website), University of Texas, March 26, 2021, https://www .mdanderson.org/cancerwise/does-immunotherapy-treat-breast-cancer.h00 -159385101.html.
Sometimes, if you’re lucky, something comes into your life just when you need it the most. That was my introduction to The Bloggess (aka Jenny Lawson aka Amazing/Funny/Fabulous human being). I LOVED her first book, Let’s Pretend This Never Happened (A Mostly True Memoir), gifted to me by my BFF. If you haven’t read it, treat yourself. Her other books are just as poignant, engaging, and hilarious. They’re like Pokemon – gotta catch them all! Or maybe potato chips – betcha can’t read just one. Something like that.
Better yet, grab the Audiobook! Jenny narrates it, and the humor and heartache and hope just flows from her voice directly to your brain cells, releasing serotonin and making you feel better no matter what you’re going through. Which brings me back to my first point – the something-that-comes-into-your-life-just-when-you-need-it-the-most point:
Shout out to @TheBloggess for keeping me company (via audiobook) through two breast biopsies today. You be funny! And awesome!
— Dana Brantley-Sieders, Ph.D. (@DBSieders) May 17, 2018
Yes, I am a fangirl and yes, I show love to show my appreciation!
The day I endured two breast biopsies was a bad day. It would have been worse without Jenny, who allowed me to escape into her world and kept me company while I was waiting to go on the slab. And guess what?
SHE FOLLOWED ME BACK ON TWITTER!!!!
This was the highlight of my year, people! It also kept me going and inspired me while writing Talking to My Tatas. Jenny’s story touched and inspired millions, and she’s saved lives, y’all! I wanted to do the same. Whenever I got frustrated, stuck, or wanted to just give up on the writing, querying, and rejections, I remembered Jenny.
Fast-forward to the present, and guess what? Jenny Lawson endorsed my book!
“I don’t know much about cancer, but I know good writing and humor, and Dana Brantley-Sieders has those in spades.” — Jenny Lawson, #1 New York Times-bestselling author of “Let’s Pretend This Never Happened”
I’m delighted, grateful, and I’m totally going to stalk visit her at The Nowhere Bookshop someday soon. Thanks, Babe!
Talking to My Tatas: A Breast Cancer Researcher’s Adventure With The Disease And What You Can Learn From It is scheduled to be published February 8, 2022!
On. My. 49th. Birthday.
I’m not one for signs, but this is the second serendipitous date associated with this book baby so far. The first was getting the offer for publication from Rowman & Littlefield on November 5 of last year, the same day I was in surgery for the first step in my left breast reconstruction. This is the second. I am filled with joy and delight!
What’s next in the process? Now that I’ve turned in finalized chapters and other components of the book with edits in response to super helpful comments and notes from editor Suzanne Staszak-Silva (shout out to my amazing literary agent Barbara Collins-Rosenberg for giving me edits and notes prior to sending them to Suzanne), the manuscript enters the production phase. I’ll be receiving notes from the Production Editor, completing any revisions, going through proofs, reaching out for endorsements – shout out to the folks who already said, “Yes, send it to me for an endorsement!” – and planning for the release and promotion.
I cannot WAIT to see the cover!
I also cannot wait until this book is available to the public, including the hundreds of thousands of newly diagnosed breast cancer patients, current patients, survivors, and caregivers. If I can help even one of those people – my survivor sisters and brothers – by informing them, inspiring them, helping them cope, or giving them a much needed laugh, then I will have accomplished something really special.
This book will also help me develop a guide for newly diagnosed breast cancer patients at my institution, another labor of love.
I send love and gratitude to all of the mentors and colleagues who’ve made me into the scientist I am today, my healthcare team for saving my life and helping me thrive, and my family for being my strength and limitless supply of love.