Use the promo code 22JOYSALE at checkout to get the sale price now through January 6, 2023!
This is a great deal, as you’ll save over $12 on the Hardback and almost $12 on the eBook. Know someone who is going through breast cancer? This would be a helpful gift. Know someone who’s a science loving nerd? They’ll probably like it, too!
I’m so excited to share news about my new job with the Susan G. Komen Foundation! It may come as a bit of a surprise to those who’ve been following my blog and slices of science and life as a scientist. Why leave research? Well, I actually haven’t left research. I’m just doing a different kind of research. More on that later, but first, why the change? As with any big life decision, there were a LOT of contributing factors. Some of the most important include:
Having an Immediate Impact on Patients and Survivors
I love research, value my time in the laboratory, and appreciate every project I had the opportunity to lead or contribute to in some way. I commend and support my colleagues, especially those who will continue my projects in the lab and build on them to make great strides. Since becoming a survivor, however, something was missing for me. I hope something I’ve done in the lab makes it to the clinic someday, but there’s no guarantee. As a survivor, it’s really important to me to make a difference now. At Komen, I’ll have that opportunity. And I’ll also have the opportunity to support Komen Scholars and grantees conducting research! Since I’ll be coding funded grants (click here for more on Common Scientific Outline [CSO] codes) to capture data, which involves reading applications, I’ll also be able to keep up with the latest advances in the field – advances that I can share with my followers and readers here!
100% Remote Work
Me in my Home Office! Photo Credit Patrick Sieders (a.k.a. Hubby)
This is so great in the age of Covid! I want to protect my health and the health of my loved ones, so being able to work from home minimizes my risk of exposure to the SARS-CoV-2 virus and all its variants. Since I no longer have a commute, I’m saving on gas (and cutting my carbon footprint), can hit the ground running by simply turning on my computer and starting my work day, and I can be more efficient and focused. My furry office mates are great company, and I can eat healthier from home and carve out more time for exercise. No excuses!
Also, with 100% remote work, the job can move with me! My husband and bought land in North Carolina for our dream home last year. We haven’t been able to break ground yet due to ongoing supply chain issues and high prices (Thanks, Covid), but it will happen soon. I didn’t want to be moving while looking for a new job at the same time. Don’t have to worry about that now!
Work/Life Balance
Academic Research is very rewarding and has a lot of pros: flexibility, freedom to pursue a myriad of research directions (so long as you can get funding), and being the first to make a new discovery or push the field forward, to name a few. But there are also challenges. The struggle to acquire funding and increasing competition as funding is limited creates a great deal of stress, not to mention long, long hours generating new preliminary data and preparing new grant applications. Before I left, I submitted three grant applications in the space of two months, and it took a toll on me physically and mentally. It also took me away from the things I love about research, like actually doing experiments, mentoring, networking and collaborating, and it took away so much personal time and time with my family. In academia, you’re never really “off.” You’re constantly bringing home papers to read, answering emails after hours, performing literature searches and working on manuscripts before and after dinner and family time, and often working into the wee hours of the morning. At this point in my life and career, I wanted and needed a better work/life balance – as a human being, as a parent, as a caregiver for aging parents – I needed to stop burning my candle at both ends. Komen is all about work/life balance.
Career Growth and Learning New Skills
As a Research Evaluation Manager, I’ll be tracking the impact of Komen funded research in many areas, including products like biomarkers and new drugs, clinical trials, new interventions, and career progression and trajectories for Komen-funded investigators using data collected by amazing colleagues since the early 1980s. The data are so rich and informative, a veritable history of progress in breast cancer research and milestones in treatments. I’m so excited to dig in! I’ll also be involved in adding to the data by coding newly funded grants, as well as evaluating the impact of research and programs sponsored by Komen. There are a wealth of opportunities, and I’m excited to be a part of it!
I’m also stoked about opportunities in communication and outreach! As a writer and communicator with a mission to bring accessible science to the public, this is my jam! I’m hoping to use the skills I honed from writing Talking To My Tatas to be a vocal and effective ambassador for science and liaison between researchers and stakeholders.
A Mission and Community I Believe In
The mission of Susan G. Komen is to save lives by meeting the most critical needs in our communities and investing in breakthrough research to prevent and cure breast cancer. Everyone working at Komen is 100% committed to this mission, which is patient and survivor focused. It’s not just lip service – many of the colleagues I’ve met in my first week are breast cancer survivors or have been directly impacted by breast cancer through friends, family, and loved ones diagnosed with breast cancer. I feel comfortable sharing my story and feel a deep sense of connection and common purpose when I hear the stories of my colleagues. It makes the work so meaningful. I believe in it, and I’m committed to giving it my all to be a part of the solution to the huge problem that is breast cancer.
Strapped for cash? There’s still plenty you can do. If you know someone going through cancer treatments, reach out. Bring food or groceries, Zoom/Skype/FaceTime and chat to give that person a bit of company and sense of normalcy. In these times, believe me, it helps. Everything, even seemingly small things, help.
Originally Published in VICC Momentum September 23, 2020 | Dana Brantley-Sieders, PhD
Note: This is an essay I wrote last summer. Though my journey continues thanks to residual disease and a mastectomy after I submitted the essay, the spirit and information in the essay hold true. I have hope. And I’m still working hard to fight cancer inside the laboratory and out in the wider world.
I had been studying breast cancer for more than 20 years when I was diagnosed with invasive ductal carcinoma. My professional life was filled with hours of watching tumor cells grow and spread on plastic dishes, marveling as they branched and blebbed in three-dimensional matrices, monitoring the size of lumps from spontaneous or transplanted breast tumor tissue in experimental mouse models, and if I was lucky, watching their growth slow or even seeing them shrink when a new experimental therapeutic worked in pre-clinical testing.
Over the years, family and friends had come to me for information, reassurance and comfort in the face of their diagnoses. I’d lost a close cousin to the ravages of aggressive breast cancer. She was only 37 years old.
When my mother was diagnosed with breast cancer, I emptied her surgical drains after her double mastectomy, caring for her with a toddler clinging to my leg and a baby balanced on my hip. I brought meals to a close friend who was diagnosed with stage 3 breast cancer, visiting with her as she endured chemotherapy, surgery, reconstruction, and finding her new normal while our pre-teen daughters hovered in the background, their infectious laughter a balm to the devastation wrought by the big “C.”
After all of this, I thought I knew breast cancer. Then it kicked me in my left breast and flung me, bleeding, on the curb of uncertainty. Turns out, I had a lot to learn.
When Brent Rexer, MD, my medical oncologist, walked in to my first appointment at the Vanderbilt Breast Center, he greeted me with kindness and a wry smile. “It’s good to see you again, though I wish it was under better circumstances.” I’d known Brent for years. He and his wife were classmates of mine in graduate school, and we’d crossed paths at research seminars in the Vanderbilt-Ingram Cancer Center. I’d crossed paths with many of the clinicians and providers who would become a part of my care team. I was lucky. I knew I was in great hands.
When I got cancer, I came home.
What did I learn from the laboratory bench to my own bedside? For starters, I learned that nothing, not even a career spent tackling this disease, can prepare you for your own diagnosis. I was as shocked, devastated, and numb as any woman who hears those three terrible words — you have cancer.
I learned that radiologists save lives. The radiologist who spotted the suspicious spot on a routine mammogram and later during an ultrasound examination has over 30 years of experience in the field. Because I’m a geek, I always ask to see what’s going on in any exam. I’m “that patient,” the one who’ll ask if I can look at the computer screen after a boob squeeze, à la mammography, and in the middle of having the goo-covered wand gliding over my exposed boob during an ultrasound. When I had the chance to look at my tumor and a previously detected benign lesion side by side, I realized that this radiologist’s years of training and sharp eyes (that could tell the difference between two grainy spots on an ultrasound that looked the same to me) caught one tumor before it could become immediately life threatening. We later learned that I had two tumors of the same subtype in the same breast, which is pretty rare. But we would not have caught the smaller one, which was actually growing faster, had my radiologist not spotted the larger mass.
I learned that I had the option of saving most of my breast tissue. Thanks to years of study following outcomes of patients who chose lumpectomy and those who chose mastectomy as surgical options, we know that choosing breast conserving surgery does not increase a woman’s risk for distant recurrence. There is an increased risk for local recurrence, but that can be mitigated with radiation therapy. I was fortunate enough to be a good candidate for partial mastectomy followed by oncoplastic reconstruction, which is essentially a breast reduction and lift. I’m not going to lie – it’s like being 18 again. I’m perky! Better still, it preserved sensation in my breast skin and nipples, and the recovery time was much shorter than with a mastectomy. Note: there are no wrong choices, only informed choices. The decision to keep or remove one or both breasts after a cancer diagnosis is a deeply personal one. Each individual patient must consider the options, the benefits and risks, and decide what is right for her. This was the best decision for me, and I’m glad I was a good candidate for this surgical option.
I learned that surgeons are brilliant, and by working together, they can give you back much of what you lost. My surgical team, including Ingrid Mezoely, MD, and Galen Perdikis, MD, worked together on a plan that allowed Dr. Mezoely to remove my tumors and Dr. Perdikis to perform oncoplastic reconstruction just after. A year and a half later, I am pleased with the result, like the way I look and feel, and while I’ll never be the same as B.C. (before cancer), my new normal is better than I ever imagined.
I learned that radiation therapists are some of the nicest, funniest people on the planet. My go-to coping mechanism is humor. When I came in for a dry run prior to my first radiation therapy, the technician placed several markers on my left breast in order to properly align the beam for more precise targeting of the area where the tumors were removed while minimizing potential damage to my heart and lungs. The shiny markers formed a cute little circular pattern, so I joked that we could make it into a pastie. All I need would be some glitter and a tassel. We both cracked up, and I was able to relax, hold my breath for the designated time, and get prepared for my treatment course. During those visits, I talked with the therapists and Bapsi Chakravarthy, MD, about topics big and small — kids, work, life, research, politics, favorite books and television shows, and all manner of topics that made the discomfort during the last weeks of treatment much more bearable.
I learned the depths of compassion and generosity of my colleagues, both in the laboratory setting and in the clinic. Disclosing a cancer diagnosis to your employer and co-workers can be frightening. Will you be at risk for losing your job (a reality for too many Americans)? Will your colleagues see you and treat you differently? Will moving forward be awkward, with colleagues feeling uncomfortable and at a loss for words? I was lucky and found support and comfort, with offers to help keep the research in my laboratory going while I was out on medical leave, with encouragement, and with the honor of serving as a reminder of what all of us in cancer research work for — helping patients diagnosed with cancer survive and thrive.
I learned that, having been on both the research side and patient side of the breast cancer experience, I have a unique perspective and the opportunity to help people outside of the laboratory. Scientists are very good at communicating with one another within the research community, but I believe we need to expand our efforts to communicate with the public. After all, most of us are funded by the National Institutes of Health, which is in turn supported by tax dollars. I feel an obligation to be able to explain my work and why it’s important to anyone who asks, be it my 11-year-old son or a person sitting next to me at the airport. I have a new mission: to be an advocate for science and bring science to the public, particularly when it comes to breast cancer. Sadly, we live in an age of fake news and pseudoscience, made worse by the pervasive anti-intellectual and anti-science political culture gripping the United States and much of the world. The internet and social media are plagued by scammers selling “alternative medicine” and woo woo “cures” for cancer. Knowledge is power, and lack thereof can be deadly. I can lend my voice to fighting myths and scams for the public good through speaking, blogging and writing.
I learned that there will be good days and bad days, and that it’s OK to seek help. My prognosis is great, but my type of breast cancer can recur years or decades after surgery and treatments are complete. That thought often keeps me up and night and serves as a source of worry. Shortly after my diagnosis, I worked to the point of exhaustion in the lab, at home, and on my side gig, staying up late in the name of productivity and maximizing creativity, but I wasn’t fooling anyone. I was terrified. After a year and a half of ups and downs, I acknowledged that I was not fine, and that I needed help in the form of therapy. I’m glad I did. Tackling my fears and anxieties head on has helped me be my best self, accept my new normal as a cancer survivor and focus on living the life I have with joy and purpose. And when I go back into the well of despair, as many survivors do, I now have the tools to climb back out and get back on track, which is very empowering.
Finally, I learned that I’m still learning. I have the best job as a researcher in that I get to be a lifelong learner. So many strides have been made since I entered the field, when Herceptin was first developed for HER2-positive breast cancer. Now, we have so many new tools in diagnostics and prognostics (3D mammography and OncoType DX testing), treatments (aromatase inhibitors, CDK inhibitors, and immune therapy), and amazing new treatments on the horizon. We still have so much work to do, but we are making a difference, and I am privileged to be a part of that process.
Medical students and their mentors in MCN
Medical Scholar conducting breast cancer research in Dr. Dana Brantley-Seider’s lab for Medical Scholars Program
Vanderbilt University Medical Center
Photo: Anne Rayner; VU
This year I have the great fortune of mentoring a talented and dedicated medical student in my lab, Kalin Wilson. Her interest is in oncology, so it’s a great fit for my ongoing and new research directions. She’s working on two projects with similar goals: to identify and characterize new drug combinations and new experimental therapeutics for triple negative breast cancer in pre-clinical studies. This is an urgent unmet need in the clinic. Triple negative disease is a subtype of breast cancers that do not express hormone receptors (estrogen receptor and progesterone receptor) or cell surface HER2 (amplified in ~25% of breast cancers). These receptors are druggable targets, and their absence limits treatment options for patients with triple negative breast cancer to surgery, radiation, and chemotherapy. Triple negative breast cancers are aggressive and disproportionately affect young women and women of African descent. Our goal is to find molecular targets for new drugs to give women with this type of breast cancer more and better options.
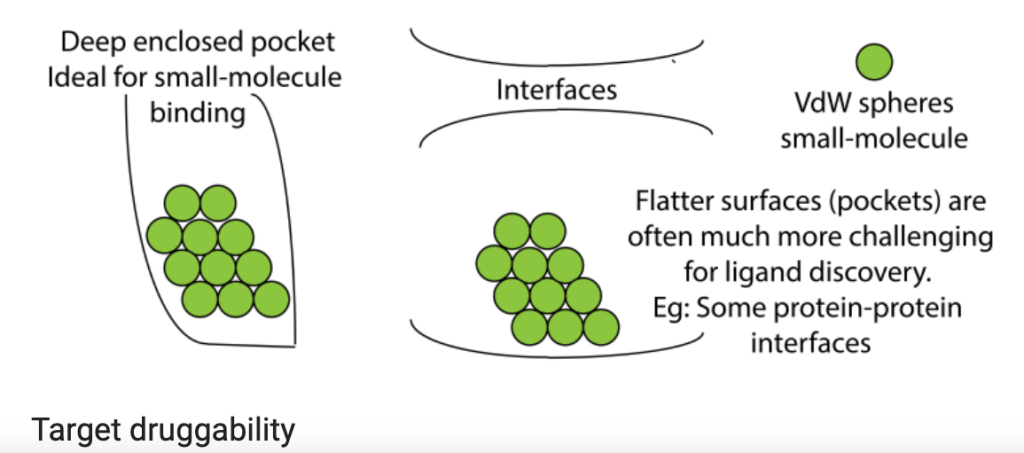
My student’s primary project is to test nanoparticle delivery systems to transport gene therapy to tumors. Many of the genes that drive cancer code for proteins that aren’t easily druggable by small molecules that fit neatly into a unique structural region in the target protein to block its function (e.g. deep enclosed pocket versus flat, relatively uniform interface or surface, as shown in the figure above). But what if we could stop production of cancer-driving proteins at the level of gene expression? This is actually possible in the laboratory setting in a process that exploits messenger RNA, the protein-making instructions that are copied from DNA and used by protein producing cellular machinery (see figure below). The use of small interfering RNA (siRNA) gene therapy, which causes the messenger RNA that encodes the protein’s blueprint to be destroyed, can theoretically stop production of any protein, which would make any target druggable. One of the challenges, however, is delivery of siRNAs to tumors. siRNAs tend to be unstable, so they can be easily destroyed by immune cells or taken up by the liver or kidneys as a part of their normal clearance functions. To overcome those delivery barriers, many biomedical engineers are applying nanotechnology, designing nanoparticles that surround the siRNA molecules. These nanoparticles shield and protect the siRNAs in circulation and can be modified to help homing to the tumor. In collaboration with Dr. Craig Duvall, we are testing nanoparticles delivering siRNA to destroy the blueprint for Rictor, a protein that we believe is essential for tumor cells to grow and prevents them from dying when they’re supposed to. Results so far are promising!
What I hope to give Kalin is a research experience that feeds her passion for science and drug discovery, to foster her natural skills and curiosity, and to keep striving for the goal of bench-to-bedside translational research. What she’s given me is her clinical perspective, something that has enriched my research and inspired me to do more directly translational research with the goal of clinical application. She’s also given me the gift of fearlessness and enthusiasm, which young scientists always possess in abundance and, fortunately, is contagious. The rewards of mentoring the next generation of scientists are many, but the synergy between experience (mentor) and fresh ideas and perspectives (mentee) is perhaps the most valuable.
I love you with all my boobs. I would say my heart, but my boobs are bigger
Dr. Dana Brantley-Sieders, Ph.D. (photo credit Lillian Boeskool)
I’ve spent twenty years working as a biomedical breast cancer researcher. Then, I was diagnosed with breast cancer. I thought I knew breast cancer before it whacked me upside my left boob and left me bleeding on the curb of uncertainty. I thought I knew cancer. I had a lot to learn. The purpose of this blog is to share my personal adventure with breast cancer, from the laboratory bench to my own bedside, and to provide accessible information about breast cancer biology for non-scientists. I say adventure, because I’d rather think of it as action movie with some really cool side quests instead of another tragedy-to-triumph saga. I’m not big on sagas. I am big on kickass intellectual badassery, pathological nerdiness, and talking about my sweet, sweet rack.
I’ll be posting about breast structure and function, how breast cancers arise from normal breast tissues. Notice I wrote “cancers” instead of “cancer.” Breast cancers are a actually a collection of diseases, and all breast cancers are different. To date, there are at least 5 subtypes, and subtypes within those subtypes.
It’s complicated, which is one reason why we haven’t cured these diseases. Another reason is how tricky and adaptable cancers are by their very nature. We’ll get into all of that in a few posts. In the meantime, let me get into the other purpose of this blog: fighting pseudoscience and scams with peer-reviewed, vetted science.
We live in an age of fake news and pseudoscience, made worse by the pervasive anti-intellectual and anti-science political culture gripping the United States and much of the world. The Internet and social media are plagued by scammers selling “alternative medicine” and woo woo “cures” for cancer. Through TALKING TATAS, I offer accurate, evidence-based science that is accessible to laypersons, including the more than three hundred thousand individuals diagnosed with breast cancer every year*, their caregivers, and their loved ones. Submit questions, ask for follow-up on any and all posts, be a part of the discussion. Knowledge is power, and it can save lives!