I learned so many new things today at Patient Advocacy Orientation! My best days are when I’m learning new things. It’s one of the things I love best about being a scientist, and it’s a great foundation upon which to build for my new work as a Patient Advocate.
What exactly are advocates and what do they do? In terms of Research Advocacy Programs, advocates are disease survivors (cancer survivors in my case), caregivers, and members of the community who provide the patient perspective to researchers to help shape the nature and direction of cancer research and patient care. Their role is critical, as they serve as a voice for patients, helping investigators tailor their research with patients concerns in mind – not just in terms of outcomes and sound science, but also in terms patient comfort, respect for patient rights and dignity, and beneficence. This means making sure the goals of research are focused on and aligned with serving patient needs and improving outcomes and quality of life.
This seems pretty intuitive, and I believe most investigators are truly committed and passionate about doing research that will make a difference, be it developing new treatments, better diagnostic tools, reducing side effects of existing treatments, and improving survival and quality of life for patients. I certainly was and am. But most investigators don’t experience what patients do – except in cases like mine where researchers become patients and survivors. My experience certainly changed my perspective, which is why I want to share what I’ve learned with both the research and survivor communities.
That mission became more urgent for me today in the face of some jarring statistics. Tennessee and the surrounding regions have some of the highest cancer death rates in the United States.
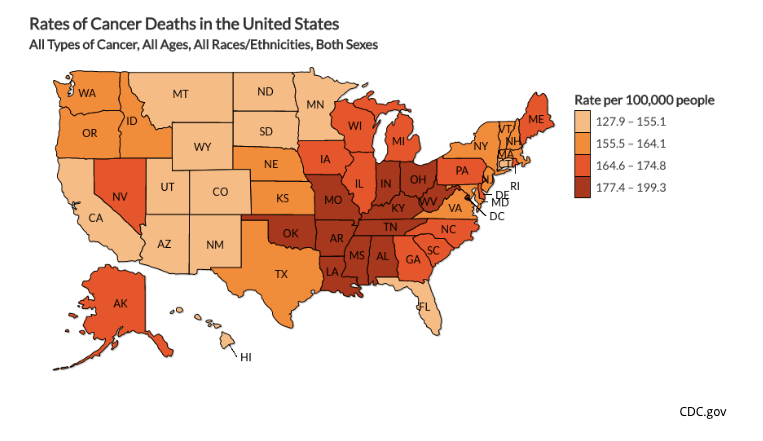
Comparing the map above to the map below that shows new cancer cases diagnosed by state, incidence, the frequency with which cancer occurs, doesn’t fully explain higher death rates.

My heart sank when I saw these data, and really drove home my privilege. I am well-educated, have a high socioeconomic status, have access to insurance coverage and some of the best health care available in the United States, and I have inside information based on my work as a breast cancer researcher.
I’m lucky. Far too many of my fellow Tennesseans and Southerners are not. My Institution and Affiliated Cancer Center serve this region. I want to be a part of better serving patients in this region, which will be a HUGE focus of my advocacy work.
What will this work involve? One of the ways I think I can be of use is by helping recruit patients for clinical trials. According to what I learned today, many promising new drugs do not make it through Phase III clinical trial testing* due to failure to accrue enough patients to sufficiently test their effectiveness. That’s such a shame and missed opportunity. Of course, there are many barriers for patient participation in clinical trials – fear/lack of understanding; lack of access due to barriers to travel/transportation, unmet childcare needs, inability to take time off work, etc.; disparities that make minority populations reluctant to participate**. While I am not in a position to combat access to trials, I am in a position to serve as a liaison between patients and clinical researchers accruing patients for trials. I can help educate potential trial participants in the process, assure them of their rights (including the ability to stop participating at any time), alleviate fears through helping patients understand the benefits and how they might be helping a great number of future cancer patients. I am also working with African American advocates and other advocates of color to understand and be sensitive to those communities, their histories, and their needs.
Those needs are great, particularly in terms of breast cancer outcomes. African American women diagnosed with breast cancer have lower overall survival rates compared to white women. Finding out why is crucial for closing the gap. Increasing African American participation in clinical trials is a key part of that process.

For more on cancer disparities across ethnic groups, click here.
Bottom line: I’ve got work to do, and I’m excited to work with my fellow survivors to help patients now and in the future. Interested in becoming an advocate? Here are some resources that can help! My Institution’s Advocacy Resources, How Patient Advocates Help Cancer Research: Expert Q&A, Why Patient Advocacy is Vital.
*I’ll cover clinical trials in more detail in a future post. Click here to learn more now. Phase III trials test drugs that have already been proven safe and promising in terms of effectiveness.
**African Americans remember the horrific abuses perpetrated by scientific investigators, including those in charge of Tuskegee Study of Syphilis – which resulted in hundreds of African Americans being denied treatment in order to study the long term effects of untreated syphilis